











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo

 Permalink
Permalink
Coronavirus disease 2019 (COVID-19) pandemic is an underway international public health emergency currently active in 188 countries and territories (Dong, Du & Gardner, 2020). COVID-19 first imported cases in Mexico were confirmed in late February 2020, and by March 18 first death was registered. According to Mexican General Health Council (GHC), there are three phases: a) Phase one: viral import; b) Phase two: community transmission; and c) Phase three: epidemic. On April 21 of 2020, with 8,772 confirmed cases and 712 deaths, the GHC announced that Mexico had entered phase three of the emergency plan. Mexican Health Secretary (Secretaría de Salud) then implemented several strategies to prevent and contain the contagion among the population, such as stricter health protocols, increased social distancing measures, and temporary closure of schools and workplaces. By this time, a large part of productive and social activity declined significantly.
Large-scale health emergencies can cause emotional and psychosocial disturbances in the population, triggering psychosomatic symptoms (Huremovic, 2019). Preventive and restrictive measures can cause high levels of psychological burden (Holmes et al., 2020; Pedrosa et al., 2020) and the appearance of symptoms of anxiety, depression, and stress (Rubin & Wessely, 2020; Brooks et al., 2020). It has been identified that gender, age, employment status (Y. Wang, Di, Ye, & Wei, 2020; Mazza et al., 2020; Paulino et al., 2020), auto perceived knowledge and safety, and contact with COVID-19 patients (C. Wang et al., 2020) are associated factors of either depression, anxiety, or stress symptoms among the general population. This study aimed to estimate the level of depression, anxiety, and stress; and identify the associated factors of these psychological responses during the third phase of the COVID-19 health emergency in a sample of the Guerrero State population in Mexico.
Methods
Design of the study
We conducted a cross-sectional online survey with a snowball sampling strategy. The survey was disseminated between May 11 and 18 of 2020, during the third phase of the COVID-19 health emergency in Mexico.
Participants
We included participants over the age of 18 that confirmed Guerrero State residency, participants that did not match these criteria were excluded. Records with more than 10% of missing or invalid data were eliminated. We reached 1006 Guerrero state Mexican residents between 18 and 81 years old. From this number, 997 (99.1%) accepted to participate, gave their informed consent, and completed the online survey. The final sample consisted of 666 females (66.8%) and 331 males (33.2%).
Measurements
We generated an online questionnaire designed to gather participant's sociodemographic data. Disease concern-related variables include following social distance recommendations, being part of risk population, perceived level of information about COVID-19, auto perceived safety to disease, recent contact with suspected or diagnosed COVID-19 patients, and heavy alcohol intake within the last seven days were also inquired.
Depression, Anxiety, and Stress Scales (DASS-21):
As in other mental health studies about COVID-19 psychological responses (Cortés-Álvarez, Piñeiro-Lamas, & Vuelvas-Olmos, 2020; Mazza et al., 2020; Paulino et al., 2020; C. Wang et al., 2020) we used the 21 item Depression, Anxiety and Stress Scales. This instrument is a self-report questionnaire consisting of three subscales, each composed of 7 items. Respondents score the items on a scale from 0 "did not apply to me at all" to 3 "applied to me very much." We used the original cut-off points (Lovibond & Lovibond, 1996) because standard scores are not available for the general Mexican population. A score of ≥10 points was considered positive to depression, being its severity classified as mild (10-13); moderate (14-20); severe (21-27); and extremely severe (≥28). Anxiety was identified from ≥8 points and its severity classified as mild (8-9), moderate (10-14), severe (15-19), and extremely severe at ≥20. Finally, a score of ≥15 points was considered positive to stress. The severity of stress was classified as mild (15-18), moderate (19-25), severe (26-33), and extremely severe (≥37).
Alcohol Use Disorders Identification Test - Consumption (AUDIT-C):
Heavy alcohol intake was measured with the AUDIT-C, a shortened version of the WHO's AUDIT-10 instrument (Barbor, Higgins-Biddle, Saunders & Monteiro, 2001). The AUDIT-C is a brief alcohol screening instrument that identifies hazardous drinkers and heavy episodic drinking. A sum score of 3 or 4 for women and men is considered positive to heavy episodic drinking (Cortés-Tomás, Giménez-Costa, Motos-Sellés & Sancerni-Beitia, 2016).
Ethical considerations
The Research Committee approved this study of Guerrero State's Health Services (CISSG-08-20). The first page of the survey included a digital informed consent describing the study's objectives and the use that retrieved information would be subject. Such digital informed consent had two option boxes to either consent or decline to participate. It was explicitly mentioned the confidentiality of the participation and the liberty of the participants to stop answering at any time without any restrictions.
Procedure
As Mexican National Health Council recommended social distancing, we used Google's online survey application Google Forms. A short text message containing information about the title, the study's aim, the selection criteria, and the benefits of the participation was redacted, and a blank form of the survey was attached to it. The questionnaire was first disseminated via social media and instant messaging services to collaborators, fellowship holders, and students who were asked to share the survey within their family, social and academic networks to be distributed and replicated among their contacts.
Statistical Analysis
The raw answers database was downloaded from the Google Forms platform as a comma-separated values file. All answers were recodified to either numerical or categorical variables in a dBase file. We performed the data analysis using CIETmap, open-source software that provides a graphical user interface of the R statistical programming language (Anderson & Mitchell, 2002). We obtained simple frequencies and conducted a bivariate analysis to explore factors potentially associated with depression, anxiety, and stress. The significance of bivariate associations was expressed using Odds Ratio (OR), and the statistical significance of this estimation was assessed with Mantel-Haenszel chi-square (x2mh) (Mantel & Haenszel, 1959). We also calculated the 95% Confidence Intervals (95% CI) and statistical significance (p<0.05). Finally, we conducted three multivariate analyses using a general linear mixed model for each psychological distress outcome. The initial saturated model included all statistically significant variables associated with the outcomes in bivariate analysis. Then we used a step-wise deletion of the least significant association until only significant associations remained. Finally, we tested for effect modification with the Woolf chi-square test for heterogeneity (x2het) (Woolf, 1955).
Results
A total of 1006 Guerrero State residents were reached and invited to participate in the study; 9 declined to participate, 997 gave their informed consent and finished the survey. The mean age of the sample was 35.3 years (SD 12.9). Table 1 shows that most participants were female (66.8%), Follows COVID-19 preventive measures such as keep social distancing, and stay home recommendations (80.2%), have children (46.7%), and were healthcare workers (40.5). Some 22.4% declared to be part of the population at risk. We identified that 45.8% of the sample had at least one psychological affectation.

Table 2 shows that 18.9% (189/997) of the respondents presented symptoms of depression; 21.7% (218/997) presented symptoms of anxiety, and 14.1% (141/997) presented symptoms of stress. Table 3 shows the Odds Ratio for bivariate associations with depression, anxiety, and stress.

Table 3: Bivariate associations with depression, anxiety and stress

Note: OR= Odds Ratio, CI95%= Confidence Interval 95%, * p < 0.05
Table 4 shows the final multivariate models of the factors associated with these three primary outcomes. Respondents were more likely to have depression if they were younger than 40 years, had no religion, and if they were unemployed; having children was associated with a lower risk of depression among our sample. Factors associated with anxiety were age <40 years and have had recent contact with patients suspected or diagnosed with COVID-19. Self-perception of insufficient knowledge about COVID-19 disease was positively associated with stress; individuals that reported living alone and not having children were less likely to present stress among our sample. Finally, not feeling safe of COVID-19 infection was associated with all three primary outcomes.
Table 4: Multivariate model of factors associated with depression, anxiety and stress
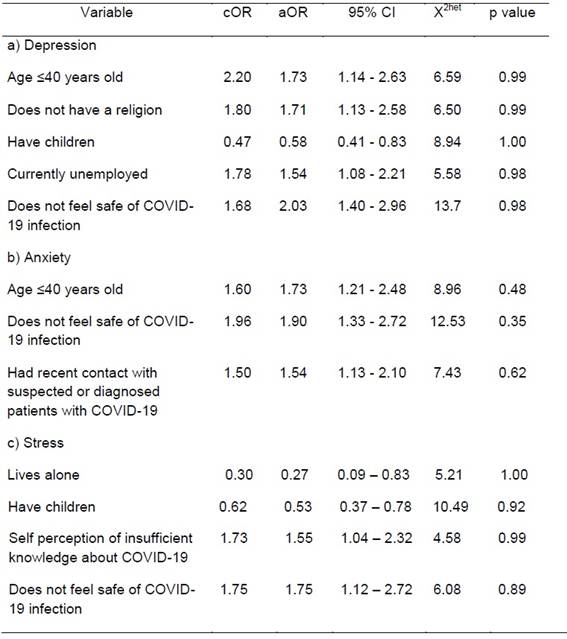
Note: cOR= crude Odds Ratio, aOR= adjusted Odds Ratio, 95%CI= Confidence Interval 95%, X2het= Woolf chi-square for heterogeneity. a: Heavy episodic alcohol did not reach significant association and was taken out from the depression saturated model. b: Self perception of insufficient knowledge about COVID-19 disease did not reach significant association and was excluded from the anxiety final model. c: Factors that did not reach significant association and were taken out of the stress final model were female gender, age ≤40 years old and currently unemployed.
Discussion
This study aimed to identify the factors associated with depression, anxiety, and stress responses during the third phase of the COVID-19 health emergency in a sample of the Guerrero State population in Mexico.
Depression, anxiety, and stress levels found in this study were lower than reported in recent literature (Mazza et al., 2020; Paulino et al., 2020; C. Wang et al., 2020) but comparable with depression levels reported by another Mexican population-based study (Cortés-Álvarez et al., 2020) and anxiety and stress levels identified in a multicentre study (Chew et al., 2020). This result could have several explanations: first, we used a validated Mexican spanish translation of the DASS-21 scales with a scoring approach based in the original cut-off points, that could have led in to misestimation of the actual frequency of depression, anxiety or stress. Second, the immediate emotional responses could have been diluted over time. The survey was set on May 11, during the third phase of the pandemic, forty-two days after the emergency declaratory by the Mexican government on March 30. Within this time-lapse, subjects could have adapted to the new, social-limited interacting reality by generating coping responses that lowered their psychological burden.
Our final model reveals that not feeling safe from COVID-19 infection is a common factor associated with depression, anxiety, and stress symptoms; this is consistent with the results in other study reporting that the perceived likelihood of contracting the disease was significantly associated with the psychological response (C. Wang et al., 2020).
In our sample, participants were more likely to present depression and anxiety if they were 40 years old or below. Mazza et al. (2020) reported that higher age was significantly associated with less depression and stress, but no significant association was identified with anxiety. It has been suggested that the young population is more likely to present information overload, a type of excess of information that leads to negative psychological responses (Rathore & Farooq, 2020).
Some studies had shown that employment status was significantly associated with depression, anxiety, and stress (Paulino et al., 2020). Our results showed that participants were more likely to present depression if they were currently unemployed. Due to GHC recommendations, non-essential activities, including the economic and productive sector, were halted in Mexico, leading to a reduction in wages in some cases and massive temporary layoffs in others. The economic crisis generated by these conditions might lead to psychological distress among those who lost their jobs.
Additionally, we found that participants who did not have a religion were more likely to present depression symptoms. It has been previously reported a protective effect of spirituality over mental health (Braam & Koening, 2019). Recent contact with patients suspected or diagnosed with COVID-19 was positively associated with anxiety symptoms. It has been reported that people who reported recent interaction with COVID-19 patients were more likely to present more psychological distress (C. Wang et al., 2020). Anxiety is an imprecise response of the body to the unknown with a feeling of escape or fight that increases at this time in the face of COVID-19 and as it spreads, feelings of sadness, lack of motivation, inhibition, and losing the desire to live to be able to arrive in extreme cases to the suicide risk (Pappa et al., 2020). Finally, our study found that participants having children were less likely to present depression. Similar to Mazza's findings (2020). On the other hand, those living alone were less likely to present stress, similar to the results of Elbay, Kurtulmuş, Arpacıoğlu, & Karadere (2020).
Conclusion
Emotional disorders, depression, anxiety, and stress, have been conceptualized over time as an excessive or prolonged cognitive, behavioural and physiological response to a situation perceived as threatening, as is currently the case with the COVID-19 pandemic, and it is even triggered by an idea about events that have not yet occurred. That perceived threat can provoke an emotional and psychophysical response. In some individuals, this reaction can be more acute if they lack of protective factors.
Recommendations
Given the epidemiological situation, health personnel must detect people with respiratory symptoms in the community and pay attention to their psychological state and well-being to take appropriate measures. Psychological well-being can become a fundamental key to the general health of the person. Although DASS-21 has been used in previous studies about COVID-19 psychological response, we recommend that future works take into account the original and validated translations of this instrument to elaborate scales that reflects health emergencies scenarios in Latin American and Mexican contexts.
Limitations
We are aware that our research may have several limitations. First, we used a cross-sectional design, which limits any causal inference. Second, due to the limited resources and national healthy distance policy, we used a snowball sampling strategy, meaning that the sample was not randomly selected. The dissemination of the questionnaire was mainly through digital messaging services and was firstly responded to by students, academics, and healthcare professionals. That could leaded an oversampling of alphabetized digital users with internet access and the participant's peer, academic and social network that may lead to selection bias; for this reason, our findings cannot be generalized among the general population but may help understand the psychological distress during the current pandemic in an educated, medium to high income and urban-based populations. Third, although psychometric properties of the DASS-21 scales have been previously analyzed in the Mexican population (Gurrola-Peña, Balcázar-Nava, Bonilla-Muños & Virseda-Heras, 2006), no evidence supports the validity of the cut-off points used in our sample. Thus, our results may not reflect the actual presence of depression, anxiety, and stress in the general Mexican population.
All the participants who had mild to extremely severe symptoms were categorized as a positive case for depression, anxiety, or stress, respectively; however, psychological responses can be divergent depending on the severity of the symptoms. We identified the risk population individuals; however, searching for specific health conditions such as chronic illnesses (i.e., diabetes mellitus or cancer) would be more effective at identifying a more detailed association.

