










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkEnfermería: Cuidados Humanizados
versión impresa ISSN 1688-8375versión On-line ISSN 2393-6606
Enfermería (Montevideo) vol.13 no.1 Montevideo 2024 Epub 01-Jun-2024
https://doi.org/10.22235/ech.v13i1.3660
Original Articles
Validation of a Brazilian Tool for Mapping Risk Factors and Early Diagnosis of Female Urinary Incontinence
1
 http://orcid.org/0000-0002-5968-0114
http://orcid.org/0000-0002-5968-0114
2
http://orcid.org/0000-0001-9297-8281
3
http://orcid.org/0000-0002-3262-9503
4
http://orcid.org/00009-0001-7559-454X
1 Universidade Regional do Cariri, Brasil
2 Centro Universitário de Juazeiro do Norte, Brasil
3 Universidade Federal de São Paulo, Brasil, luis.reis@urca.br
4 Associação Brasileira de Estomaterapia, Brasil
5 Policlínica Regional de Iguatú, Brasil
6 Faculdade São Leopoldo Mandic, Brasil
Objective:
To validate the content of the Risk Factors Mapping Instrument for Female Urinary Incontinence (IMFRIU-Fem) considering the context of young adult women.
Method:
This is quantitative methodological research, developed from April 2020 to December 2021, in three stages: integrative literature review, instrument construction and content validation.
Results:
Through the integrative review, 55 risk factors were identified and grouped into dimensions in the structure of the instrument, considering from sociodemographic aspects to body systems. The instrument was validated by the content validity index (CVI) and was assessed by 7 judges. For most of the dimensions of the instrument the judges presented a unanimous answer, expressing a percentage of 91 % as to clarity and understanding, which means that such dimensions present functionality in the face of the objective of mapping the risk factors for female urinary incontinence. The global CVI of the dimensions showed to be extremely significant, with CVI = 0.91.
Conclusion:
It is expected that the IMFRIU-Fem may help nurses to identify early risk factors for urinary incontinence, providing longitudinal data that allow the elaboration of a care plan that considers the integrality of women’s health.
Keywords: enterostomal therapy; urinary incontinence; biomedical technology
Objetivo:
Validar o conteúdo do Instrumento de Mapeamento dos Fatores de Risco para Incontinência Urinária Feminina (IMFRIU-Fem) considerando o contexto das mulheres adultas jovens.
Método:
Trata-se de uma pesquisa metodológica quantitativa, desenvolvida no período de abril 2020 a dezembro de 2021, em três etapas: revisão integrativa da literatura, construção do instrumento e validação do conteúdo.
Resultados:
Através da revisão integrativa, 55 fatores de risco foram identificados e agrupados em dimensões na estrutura do instrumento, considerando desde os aspectos sociodemográficos até os sistemas corporais. O instrumento foi validado pelo índice de validade de conteúdo (IVC) e contou com a avaliação de 7 juízes. Para a maioria das dimensões do instrumento os juízes apresentaram uma resposta unanime, expressando uma porcentagem de 91 % quanto a clareza e compreensão, o que significa dizer que tais dimensões apresentam funcionalidade diante do objetivo de mapear os fatores de risco para a incontinência urinária feminina. O IVC global das dimensões, mostrou-se extremamente significativos, com IVC = 0,91.
Conclusão:
Espera-se que o IMFRIU-Fem possa auxiliar os enfermeiros a identificar precocemente os fatores de risco para a incontinência urinária, fornecendo dados longitudinais que permitam elaborar um plano assistencial que considere a integralidade da saúde da mulher.
Palavras-chave: estomaterapia; incontinência urinária; tecnologia biomédica
Objetivo:
Validar el contenido del Instrumento de Mapeo de Factores de Riesgo para la Incontinencia Urinaria Femenina (IMFRIU-Fem) considerando el contexto de las mujeres adultas jóvenes.
Método:
Se trata de una investigación metodológica cuantitativa, desarrollada entre abril de 2020 y diciembre de 2021, en tres etapas: revisión bibliográfica integradora, construcción del instrumento y validación de contenido.
Resultados:
A través de la revisión integradora, se identificaron 55 factores de riesgo y se agruparon en dimensiones en la estructura del instrumento, considerando desde aspectos sociodemográficos hasta sistemas corporales. El instrumento fue validado por el índice de validez de contenido (IVC) y fue evaluado por 7 jueces. Para la mayoría de las dimensiones del instrumento los jueces presentaron una respuesta unánime, expresando un porcentaje del 91 % en cuanto a claridad y comprensión, lo que significa que dichas dimensiones presentan funcionalidad frente al objetivo de mapear los factores de riesgo de la incontinencia urinaria femenina. El IVC global de las dimensiones resultó ser extremadamente significativo, con un valor de 0.91.
Conclusión:
Se espera que el IMFRIU-Fem pueda ayudar al personal de enfermería a identificar de forma precoz los factores de riesgo para la incontinencia urinaria, proporcionando datos longitudinales que permitan elaborar un plan de asistencia que considere la integralidad de la salud de la mujer.
Palabras clave: estomaterapia; incontinencia urinaria; tecnología biomédica
Introduction
Urinary incontinence (UI) is defined as a complaint of involuntary loss of urine (International Continence Society - ICS, 2017) and incorporated into the International Classification of Diseases (ICD).1) It is a disorder that affects around 27 % of the world’s population and is more prevalent in women 2 due to the physical-functional transformations that occur in the female aging process, such as climacteric and menopause, making them more vulnerable to developing UI. 3
Although its occurrence is associated with aging, UI can affect women at other stages of life. In a survey of 300 women of working age, 8 % complained of involuntary loss of urine, 100% were unaware of the issue, and 54.2 % stopped going out because they were ashamed of their health condition. Studies have highlighted the increase in the occurrence of UIs in young adult women, which is a cause for concern as it has an impact on quality of life. 4
The literature points to various factors for the onset of UI in women, such as age, heredity, race, obesity, chronic diseases, pelvic floor trauma, abdominal or gynecological surgery, multiparity, urinary tract infection, medication, constipation, smoking, caffeine consumption and intense exercise in the abdominal region. 5,6
UI is differentiated into three main subtypes: stress urinary incontinence (SUI), characterized by urine loss during physical activity, coughing, and sneezing; urge urinary incontinence (UUI), when involuntary elimination of urine is preceded by an uncontrollable urge to urinate; and mixed urinary incontinence (MUI), when both types of UI mentioned above are present. 7
From this perspective, the Unified Health System (SUS) faces a challenge in seeking innovative solutions that provide comprehensive and effective care. SUS has driven health research to develop technologies and incorporate care practices based on the best evidence.8
Nurses, especially stomatherapists, are fundamental in assisting people with UIs at all levels of health care, so making resources available to these professionals to facilitate decision-making is a relevant strategy for care focused on individual needs. 9,10
Urinary incontinence, often mistakenly associated with a normal condition, becomes a silent public health problem that prevents timely diagnosis and preventative actions from being instituted, negatively impacting the physical, social, and emotional health of these women. 11 Faced with this challenging situation, the nurse’s role in prevention involves early recognition of the risk factors for urinary incontinence. Early action aims to reduce easily avoidable damage, such as exposure to surgical procedures related to UIs and drives the transformation of the current scenario.
Surgery and drugs are considered the first line of treatment for health professionals, drowning the health system with delays in solving the problem.12Early recognition of risk factors for urinary incontinence incorporates simple, low-cost, and effective preventive measures. In this way, early treatment by nurses can reduce the growth of waiting lists for specialized hospitals, direct secondary care to more complex cases, and reduce the burden on the Unified Health System (SUS) network. 13
Thus, early identification of risk factors for UI is essential to implement care, promoting the reduction of future damage to women’s health by maintaining urinary continence even in the face of physiological changes. Given this context, this study aimed to validate the instrument’s content for Mapping Risk Factors for Female Urinary Incontinence (IMFRIU-Fem), considering the context of young adult women.
Methodology
This is a quantitative methodological study carried out in three stages: 1) Literature review (LR), 2) Technology construction, and 3) Content validation with expert judges.14
The RL was carried out between April and August 2020 to list the risk factors for UI in adult women for textual production of the instrument a posteriori. The following health science descriptors were used: urinary incontinence, risk factors, and women. They were applied with the Boolean operator and in Public/Publish Medline (Pubmed) and Scientific Electronic Library (Scielo). Of the 1604 articles obtained in the initial search, the following inclusion criteria were applied: complete articles focused on the theme, with no time restriction on publication and language. We excluded articles such as letters, dissertations and theses, expert opinions, editorials, book chapters, articles that could not be accessed in full, and articles that did not answer the guiding question and did not have content related to the research topic. In addition, studies involving the elderly in general and articles that did not provide primary data were excluded. This resulted in 19 selected articles, in which 55 risk factors for UI were identified. In the second stage, the IMFRIU-Fem was structured between September and October 2020 based on the results obtained in the RL. In this stage, the factors were analyzed and grouped into dimensions, considering the sociodemographic aspects and the body systems, to enable practicality during the nurse’s investigation process.
The technology consists of two stages: the first is an instrument for investigating risk factors, and the second consolidates the dimensions and their risk factors. The instrument is organized into dimensions correlated with their risk factors, optimizing and facilitating its use. Once completed, the professional will build the patient’s risk factor panel, showing which dimensions should be focused on during the development of nursing interventions. Professionals can use this panel as a technological tool for targeted, optimized, and simplified assistance.
After drafting the instrument, the content validation stage was carried out between November and December 2021. The experts were sampled intentionally, non-probabilistically, by telephone and via WhatsApp. To be considered a suitable judge, the participant had to have experience in at least one of the following areas: stomatherapy, UI, methodological research, and/or health technologies. They were mapped using the snowball technique, as it makes it possible to build reference networks through referrals, thus constructing an intentional sample. 15
The number of judges is much debated and is of great value in measuring the quality of the instrument to be developed. Therefore, between three and sixteen judges is ideal, with a minimum of five and a maximum of ten people participating in this process. 16) Of the 15 judges identified, 11 agreed to participate in the evaluation process and signed the Informed Consent Form (ICF). However, only 7 completed all the stages. Initially, each participant answered a questionnaire via Google Forms on academic training, professional activity, and scientific production. They then received the instrument and the evaluation form, which also used Google Forms.
In evaluating the IMFRIU-Fem, a specific questionnaire was developed for this study. It was designed for the judges to assess clarity and comprehension, relevance, and the judgment of items as to whether they should be kept, not kept, or kept after changes. The instrument was validated using the Content Validity Index (CVI). It is a method that uses the Likert scale with a score of 1 to 4 points, where 1: irrelevant and 4: totally relevant. 17
The content validation index (CVI) calculation measures the proportion or percentage of judges who agree on certain aspects of the instrument and its items. It allows you to analyze each item individually and then the instrument. The index score is calculated by adding up the agreement of the items marked “3” or “4” by the experts. Items that received a score of “1” or “2” should be revised or eliminated. 16
To calculate the CVI for each item in the instrument answers 3 and 4 were added together, and the value was divided by the number of judges. Items that scored 1 or 2 and, consequently, low CVI were revised or eliminated.18CVI results ≥0.80 were considered acceptable and recommended for research with more than six judges. 16 For CVIs below 0.80, the items were excluded or reformulated. The retest is indicated for validation if the CVI is below 0.80 in the first evaluation, which was unnecessary in this study.
This study was approved by the Research Ethics Committee of the Universidade Regional do Cariri (CEP-URCA) under opinion No. 3.779.482 and Certificate of Submission for Ethical Appraisal (CAAE) 24351819.7.0000.5055.
Results
Building technology
The technology developed was supported by scientific studies compiled in a literature review. The results guided the construction of an instrument to map the risk factors for female urinary incontinence. A total of 55 risk factors were found to affect pelvic pain (Table 1).
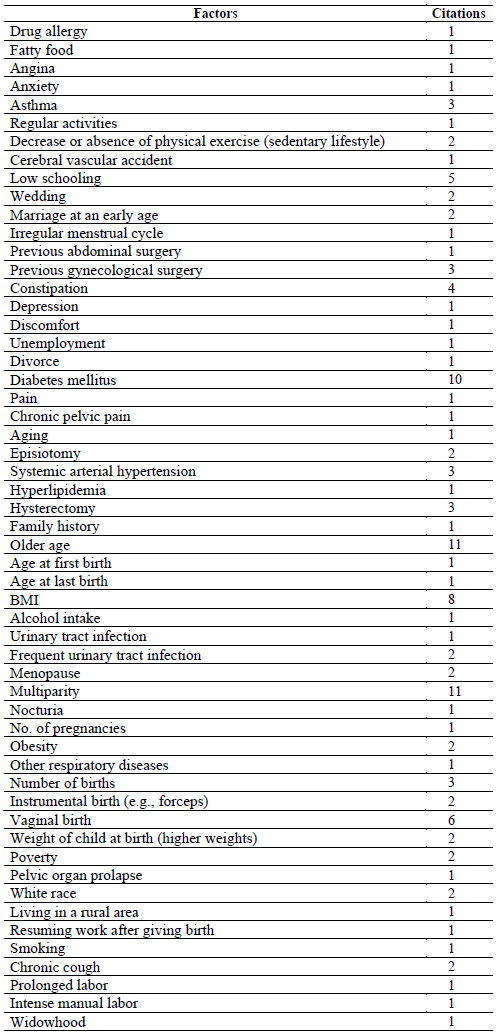
For better interpretation and analysis, the factors that were similar in meaning and the factors that more than two authors cited were organized in an Excel table, building a table of recurring risk factors, resulting in 23 risk factors (Table 2).
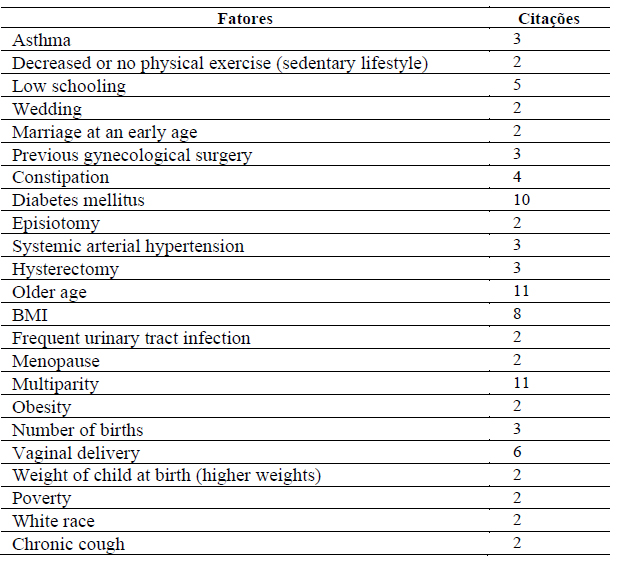
In addition to grouping them into recurring risk factors, they were regrouped into dimensions according to their affinities, making up the following: identification, sociodemographic dimension, health-disease dimension/general aspects, cardiovascular health-disease dimension, respiratory health-disease dimension, gastrointestinal health-disease dimension, genitourinary health-disease dimension, mental health-disease dimension, other diseases, symptoms and/or complaints. Therefore, the anamnesis should include elements of general identification, followed by symptomatic questioning of the various devices (ISDA), family, and personal history. 19
Technology validation
Table 3 T3 shows the characteristics of the IMFRIU-Fem judges. The sample consisted of nurses from the Northeast region, five females (71.4 %) and two males (28.6 %). The average age ranged from 20 to 59, with the 30 to 39 age group predominating (71.4 %). All the judges reported having a specialization, with the majority being specialists in stomatherapy (71.4 %). Regarding stricto sensu postgraduate studies, four had a master’s degree (57.1 %), and one had a doctorate (14.3 %).
About their working environment, five said they worked in secondary health care, one in teaching and two in both areas. Concerning scientific production, the information showed that four of the judges had already participated in dissertation or thesis boards (57.1 %), and five (71.4 %) had already authored article(s) published in the area of UI. In addition, five also revealed that they participated in research groups focusing on different areas that correlate with the theme of the work, such as: collective health, pelvic dysfunctions, stomatherapy and health technology.
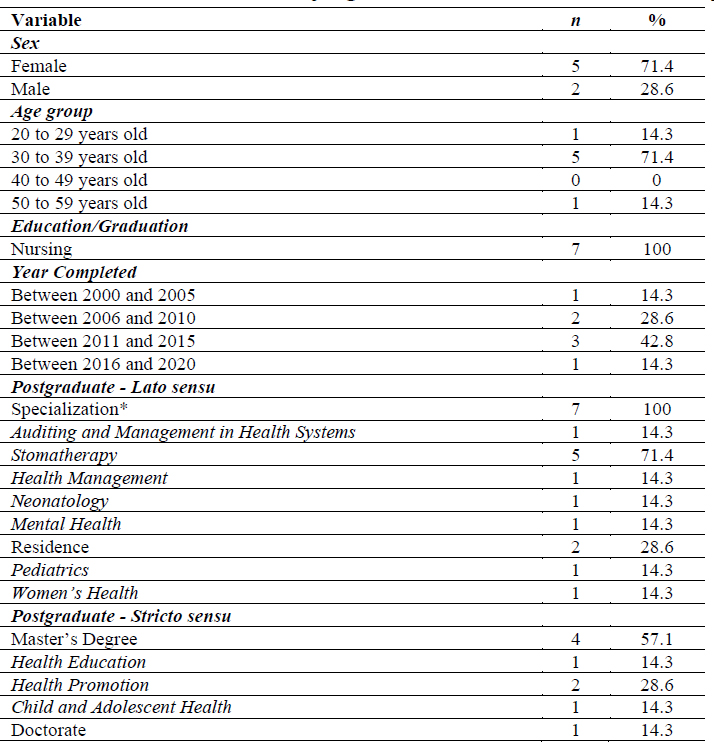
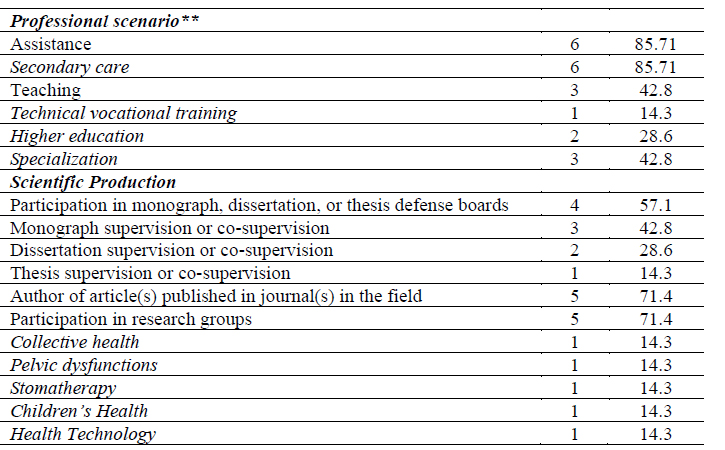
Note: *The same judge could have more than one specialization. **The same judge could act in more than one scenario
Table 4 shows the IMFRIU-Fem results regarding the clarity and comprehension of the items, the CVI per item in each dimension, and the total CVI.
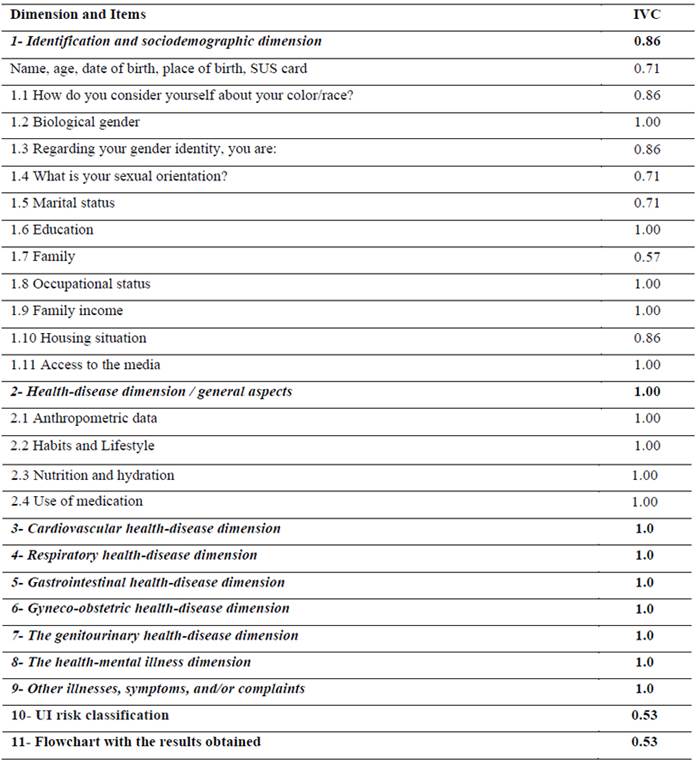
For most of the instrument’s dimensions, the judges had a unanimous response, expressing a percentage of 100 % in terms of clarity and comprehension. This means that these dimensions are functional, given the objective of mapping the risk factors for female UI. Overall, the global CVI for the dimensions was 0.91.
The identification and sociodemographic dimensions obtained a total CVI of 0.86, above the benchmark cited for exclusion. However, in the individual analysis, item “1.7 Family” had a CVI of 0.57 and was excluded from the instrument. The items “Classification of the risk of UI” and “Flowchart with the results obtained” both obtained CVIs of 0.53. In these cases, it was decided to reformulate the items in line with the evaluators’ recommendations for the final version of the instrument.
After making the adjustments requested by the evaluators, the IMFRIU-Fem instrument was exported to a QR code, which can be accessed via the camera of smartphones and tablets.F1

Discussion
The structure of the IMFRIU-Fem was designed to contemplate holism during nursing mapping. It understands that the risk factors for UI are multifactorial and not limited to pelvic floor muscle dysfunction. As identified in the literature, these range from sociodemographic aspects to mental health.
The script was intended to promote a continuous and welcoming dialog during the consultation, which was conducted according to the dimensions of women’s health. The nurse-client interaction that emphasizes active listening, welcoming, empathy, and creativity allows the person to feel part of the care process and feel able to carry it out continuously, increasing the chances of resolving the health situation. 20
The anamnesis begins with identification, followed by symptomatological questioning of the various apparatuses of the human body, family, and personal history, and finally, an investigation of gynecological and obstetric history, creating a connection with the professional and the patient. 19
Furthermore, UI, seen as a natural age process, masks the true diagnosis. Involuntary urine leakage has a negative impact on its carrier, ranging from changes in daily routines to social embarrassment, where lack of knowledge and normalization delay the search for treatment. 21 In a survey of 300 women, 24 of them said they had involuntary urine leakage, but when asked about urinary incontinence, they were unanimously unable to answer. 22
This shows that health professionals’ early recognition and identification of risk factors for developing urinary incontinence marks progress in women’s health, as leaking urine can affect quality of life. Health promotion with preventive strategies renews health care and reduces future damage to women’s health.
About the IMFRIU-Fem content validation process, it was possible to note that there was a predominance of consensus among the judges on most of the instrument’s topics, with an overall CVI of 0.91, indicating that 91 % of the experts considered the IMFRIU-Fem to be relevant for the early identification of female urinary incontinence, with the judges showing a continued interest in formulating a usable tool. The suggestions for the items with the lowest scores were considered constructive, as they allowed for a new reflection on the research focus factors for UI.
However, the family item was excluded because it resulted in a CVI value below 0.80, which was considered irrelevant for the instrument. However, the classification of UI risk and the flowchart with the results obtained, contained in the first version, received constructive suggestions, where there was an adaptation and fusion of knowledge, thus assembling the panel of dimensions correlated with their risk factors.
During the study, the highest number of risk factors related to gynecobstetric discharge was observed, strengthening the idea of building a healthy history based on preventive measures that need to be started early, impacting the maintenance of continence even with the possible damage to the pelvic floor muscles during life.
Bearing in mind that obstetric history and gynecological surgeries are considered some of the factors that alter pelvic floor function. 6 O The number of births has been identified as a risk factor for UI, with each increase in parity being associated with an increased risk of UI in women. Compared to nulliparity, the prevalence of births of two or more children is increasing, 23 and there is a history of recurrent urinary tract infections. 24
The age factor also permeates the studies, showing that those aged 36 to 50 and 51 and over have twice the risk of UI than those aged 18 to 35 and that the prevalence of UI increases with age 40 and BMI <30. 25
The body mass index is included in the general aspects section, which covers everything from anthropometric measurements to lifestyle. There is a moderate and negative correlation between anthropometric measurements and functional assessment of the pelvic floor, where these measurements are inversely proportional to pelvic floor muscle strength.26
Age, coffee consumption, a history of gynecological surgeries and recurrent lower urinary tract infections, obesity, caffeine consumption, physical activity, family illnesses, and personal history were identified as the main risk factors for urinary incontinence. 4 Added are high-impact physical activities, training duration, and intestinal and urinary symptoms, emphasizing constipation and urinary tract infections. 21 In addition, UI is considered one of the most common complications in diabetic women. 27 Risk factors that corroborate those contained in the IMFRIU-Fem structure.
A relevant point to highlight is the scarcity of technologies in female UI in Brazil. A review published in 2020 on the development of technologies aimed at women’s health in the country showed that the most covered topics were health education during pregnancy and breastfeeding. 17 No female public health policy focuses on urinary incontinence; only a discreet proposal for the elderly, which does not specify gender, is found in the policy for the elderly. 11 Given this, IMFRIU-Fem has the potential to contribute to other areas of nursing practice.
Regarding strategies to effectively enable prevention and health promotion, health technologies deserve to be highlighted due to their progressive growth over the last few years. In this sense, considering nursing specifically, the validation of consultation instruments allows new resources to be incorporated into practice to direct nursing care better and improve the quality of care for the population. 28
In the field of enterostomal therapy, adopting technologies in care can enable more effective results in the face of the different health problems enterostomal nurses face. 20 Therefore, it is worth exploring the contexts in which this nursing specialty is inserted, such as UI care.
The main limitation of this study was that it was not validated by the target audience (women with urinary incontinence). This opens the way for further studies on the reliability and efficiency of the instrument and for validating it in nursing practice in the care of female UI.
Conclusion
The process of constructing and validating the instrument was satisfactory since the overall CVI of 0.91 was achieved. In addition, in the light of the literature analyzed, it provided recognition of the risk factors related to female urinary incontinence.
Given the above, it can be inferred that the IMFRIU-Fem can be used for nursing consultations with adult women, providing systematized care to prevent urinary incontinence, raising awareness of the importance of new resources in health care that can improve people’s quality of life, prevent and promote health, and be a useful resource for planning and implementing nursing care for UI.
It is hoped that the IMFRIU-Fem can help nurses identify risk factors for UI early, providing longitudinal data that will enable them to draw up a care plan that considers the integrality of women’s health. It is also hoped that the tool can be implemented beyond Brazil, innovating the practice of stomatherapy nursing and further strengthening and consolidating this specialty.
REFERENCES
1. UFU. CID-10 Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde (Internet). Universidade Federal de Uberlândia. 2016 (acesso em 2022 Jul 1). Disponível em: Disponível em: https://bibliotecas.ufu.br/portal-da-pesquisa/base-de-dados/cid-10-classificacao-estatistica-internacional-de-doencas-e [ Links ]
2. Silva, M de M, Oliveira, ATR, Peres, MGP. Os benefícios da fisioterapia pélvica para mulheres com incontinência urinária. Revista Cathedral (Internet). 2021 (acesso em 2022 Jul 1);3(2):48-55. Disponível em: Disponível em: http://cathedral.ojs.galoa.com.br/index.php/cathedral/article/view/301 [ Links ]
3. Tomasi, AVR, dos Santos, SMA, Honório, GJDS, Locks, MOH. Incontinência urinária em idosas: práticas assistenciais e proposta de cuidado âmbito da atenção primária de saúde. Texto & Contexto - Enfermagem (Internet). 2017 (acesso em 2022 Jul 1);26(2):6800015. doi: 10.1590/0104-07072017006800015 [ Links ]
4. Mourão, LF, Luz, MHBA, Marques, ADB, Benício, CDAV, Nunes, BMVT, Pereira, AFM. Caracterização e fatores de risco de incontinência urinária em mulheres atendidas em uma clínica ginecológica. ESTIMA, Brazilian Journal of Enterostomal Therapy (Internet). 2017 (acesso em 2022 Jul 1);15(2):82-91. doi: 10.5327/Z1806-3144201700020004 [ Links ]
5. Kubiak, K, Husejko, J, Gajos, M, Wysocka, O, Lamtych, M, Modlińska, A, et al. Management of stress incontinence in older women. Journal of Education, Health and Sport (Internet). 2019 May 18 (acesso em 2022 Jul 1);9(5):209-220. doi: http://dx.doi.org/10.5281/zenodo.2898653 [ Links ]
6. da Silva, JCP, Soler, ZASG, Wysocki, AD. Associated factors to urinary incontinence in women undergoing urodynamic testing. Revista da Escola de Enfermagem da USP (Internet). 2017 (acesso em 2022 Jul 1);51:1-8. doi: 10.1590/S1980-220X2016140903209 [ Links ]
7. de Moura Brasil, DM, Nicolau, AIO, Bilhar, APM, Karbage, SAL, Lucena, SV, do Carmo, TF, et al. Urinary incontinence and female sexual function: An integrative review of validated questionnaires. ACTA Paulista de Enfermagem. 2018;31(5):558-563. doi: 10.1590/1982-0194201800077 [ Links ]
8. Fernandes, BCG, Silva Júnior, JN de B, Guedes, HCDS, Macedo, DBG, Nogueira, MF, Barrêto, AJR. Use of technologies by nurses in the management of primary health care. Revista Gaúcha de Enfermagem (Internet). 2021 May 19 (acesso em 2022 Jul 1);42(spe):e20200197. doi: 10.1590/1983-1447.2021.20200197 [ Links ]
9. Braga, F das CSAG, da Costa, AP, das Neves, NVP, da Silva, GRF, da Silva, ARV, Jorge, HMF. Tecnologias para educação em saúde no cuidado ao paciente com incontinência urinária: revisão integrativa. ESTIMA, Brazilian Journal of Enterostomal Therapy. 2021;19: e2621. doi: 10.30886/estima.v19.1122_IN [ Links ]
10. Moraes, JT, Fonseca, DF da, da Mata, LRF, Oliveira, PP de, Sampaio, F de C. Validação de um instrumento para consulta de enfermagem à pessoa com diabetes mellitus e/ou hipertensão arterial. Revista de Enfermagem Referência. 2018;19:127-136. doi: 10.12707/RIV18041 [ Links ]
11. Peres De Carvalho, M, Andrade, FP, Peres, W, Martinelli, T, Simch, F, Bueno Orcy, R, et al. O impacto da incontinência urinária e seus fatores associados em idosas. Revista Brasileira de Geriatria e Gerontologia (Internet). 2014 (acesso em 2022 Jul 1);17(4):721-730. doi: 10.1590/1809-9823.2014.13135 [ Links ]
12. Brito, FA de, Gentilli, R de ML. Desatenção à mulher incontinente na atenção primária de saúde no SUS. Fisioter Bras (Internet). 2017 (acesso em 2022 Jul 1);18(2):205-213. Disponível em: Disponível em: https://docs.bvsalud.org/biblioref/2018/05/884446/desatencao-a-mulher-incontinente-na-atencao-primaria-de-saude-no-sus.pdf [ Links ]
13. Assis, GM. Atuação do enfermeiro na área de incontinências: podemos fazer mais. ESTIMA, Brazilian Journal of Enterostomal Therapy. 2019;17:e0719. doi: 10.30886/estima.v17.761_PT [ Links ]
14. Polit, DF, Beck, CT, editores. Fundamentos de pesquisa em enfermagem: Avaliação de evidências para prática de enfermagem. Porto Alegre: Artmed; 2011. [ Links ]
15. Vinuto, J. A amostragem em bola de neve na pesquisa qualitativa. Tematicas (Internet). 2014 (acesso em 2022 Jul 1);22(44):203-220. doi: 10.20396/tematicas.v22i44.10977 [ Links ]
16. Alexandre, NMC, Coluci, MZO. Validade de conteúdo nos processos de construção e adaptação de instrumentos de medidas. Ciência & Saúde Coletiva (Internet). 2011 (acesso em 2022 Jul 1);16(7):3061-3068. doi: 10.1590/S1413-81232011000800006 [ Links ]
17. Barros, FRB de, Lima, RF da S. Tecnologias desenvolvidas no contexto da saúde da mulher no Brasil: uma revisão integrativa . Revista Cuidarte (Internet). 2021 (acesso em 2022 Jul 1);12(1):e1159. doi: 10.15649/cuidarte.1159 [ Links ]
18. Souza, AC de, Alexandre, NMC, Guirardello, E de B. Propriedades psicométricas na avaliação de instrumentos: avaliação da confiabilidade e da validade. Epidemiologia e Serviços de Saúde (Internet). 2017 (acesso em 2022 Jul 1);26(3):649-659. doi: 10.5123/S1679-49742017000300022 [ Links ]
19. Amorim, RP de, Oliveira, JS de, Machado, ALM, Chady, JN da C, Mota, AM da. Manual de Habilidades Profissionais: atenção à saúde de mulheres e gestantes. Belém: EDUEPA; 2018. Disponível em: https://paginas.uepa.br/eduepa/wp-content/uploads/2019/06/MANUAL-DE-GINECOLOGIA-E-OBSTETR%C3%8DCIA.pdf [ Links ]
20. Shoji, S, Souza, NVD de O, Maurício, VC, Costa, CCP da, Alves, FT. O cuidado de enfermagem em Estomaterapia e o uso das tecnologias. ESTIMA, Brazilian Journal of Enterostomal Therapy (Internet). 2017 (acesso em 2022 Jul 1);15(3):169-177. doi: 10.5327/Z1806-3144201700030008 [ Links ]
21. Mendonça, FF, Lima, FGS, Rezende, FR. Os impactos da incontinencia urinária nas mulheres . Revista Interação Interdisciplinar (Internet). 2022 (acesso em 2022 Jul 1);(1):2-8. Disponível em: Disponível em: https://publicacoes.unifimes.edu.br/index.php/interacao/article/view/1448 [ Links ]
22. Dantas, MA, Dias, CSB, Nascimento, EGC do. Frequência da incontinência urinária em mulheres na idade produtiva. Revista de Enfermagem e Atenção à Saúde (Internet). 2020 (acesso em 2022 Jul 1);9(2):16-27. doi: 10.18554/reas.v9i2.3521 [ Links ]
23. Zhou, HH, Shu, B, Liu, TZ, Wang, XH, Yang, ZH, Guo, YL. Association between parity and the risk for urinary incontinence in women: A meta-analysis of case-control and cohort studies. Medicine (Internet). 2018 (acesso em 2022 Jul 1);97(28):e11443. doi: 10.1097/MD.0000000000011443 [ Links ]
24. Nazzal, Z, Khatib, B, Al-Quqa, B, Abu-Taha, L, Jaradat, A. The prevalence and risk factors of urinary incontinence amongst Palestinian women with type 2 diabetes mellitus: A cross-sectional study. Arab Journal of Urology (Internet). 2020 (acesso em 2022 Jul 1);18(1):34-40. doi: 10.1080/2090598X.2019.1699340 [ Links ]
25. Komeilifar, R, Javadifar, N, Afshari, P, Haghighizade, MH, Honarmandpour, A. The Prevalence, Subtypes and Obstetric Risk Factors of Urinary Incontinence in Reproductive Age Women Referred to Community Health Care Centers of Dezful, Iran- 2015. International Journal of Community Based Nursing and Midwifery (Internet). 2017 (acesso em 2022 Jul 1);5(3):275-283. PMID: 28698886. [ Links ]
26. Mansour, KMK, Goulart, C da L, Santos, LS dos, Carvalho, L, Schuh, CM, Sudbrack, AC. Revista Pesquisa em Fisioterapia (Internet). 2018 (acesso em 2022 Jul 1);8(3):330-335. doi: 10.17267/2238-2704rpf.v8i3.1993 [ Links ]
27. Dantas, MA, Dias, CSB, Nascimento, EGC do. Frequência da incontinência urinária em mulheres na idade produtiva. Revista de Enfermagem e Atenção à Saúde. 2020;9(2):16-27. doi: 10.18554/reas.v9i2.3521 [ Links ]
28. Higa, R, de Moraes Lopes, MHB, dos Reis, MJ. Fatores de risco para incontinência urinária na mulher. Revista da Escola de Enfermagem da USP (Internet). 2008 (acesso em 2022 Jul 1);42(1):187-192. doi: 10.1590/S0080-62342008000100025 [ Links ]
How to cite: Moreira RA, de Araújo AF, Macedo LFR, Goulart ML, Bezerra MSA, Jacob LM da S. Validation of a Brazilian Tool for Mapping Risk Factors and Early Diagnosis of Female Urinary Incontinence. Enfermería: Cuidados Humanizados. 2024;13(1):e3660. doi: 10.22235/ech.v13i1.3660
Authors’ contribution (CRediT Taxonomy): 1. Conceptualization; 2. Data curation; 3. Formal Analysis; 4. Funding acquisition; 5. Investigation; 6. Methodology; 7. Project administration; 8. Resources; 9. Software; 10. Supervision; 11. Validation; 12. Visualization; 13. Writing: original draft; 14. Writing: review & editing. R. A. M. has contributed in 1, 2, 5, 13; A. F. de A. in 1, 2, 3, 12; L. F. R. M. in 1, 3, 6, 13; M. L. G. in 1, 5, 11; M. S. A. B. in 1, 8, 11, 14; L. M. da S. J. in 1, 2, 14.
Received: September 02, 2023; Accepted: March 13, 2024
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
