










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Links relacionados
Compartir

 Permalink
PermalinkOdontoestomatología
versión impresa ISSN 0797-0374versión On-line ISSN 1688-9339
Odontoestomatología vol.26 no.43 Montevideo 2024 Epub 01-Jun-2024
https://doi.org/10.22592/ode2024n43e231
Research
Pattern of shape variation of the mandibular dental arch in a sample from the Metropolitan Region of Chile
1
 http://orcid.org/0000-0001-5346-7518
http://orcid.org/0000-0001-5346-7518
2
http://orcid.org/0000-0002-9945-4656
1Cirujano-Dentista Práctica Privada, Santiago, Chile. Código postal 7650682. f.vidaurre9@gmail.com
2 Hospital de Urgencia Asistencia Pública, Santiago, Chile
3 Instituto de Investigación en Ciencias Odontológicas (ICOD), Centro de Análisis Cuantitativo en Antropología Dental (CA2) , Facultad de Odontología y Departamento de Antropología, Facultad de Ciencias Sociales, Universidad de Chile, Santiago, Chile.
4 Servicio de Cirugía Máxilo Facial, Hospital San Borja Arriarán. Departamento del Niño y Ortopedia Dento Maxilar, Centro de Análisis Cuantitativo en Antropología Dental. Facultad de Odontología, Universidad de Chile. Santiago, Chile.
Objectives:
Describe the pattern of shape variation of the mandibular dental arch in a sample from the Metropolitan Region through an observational, cross-sectional study.
Methods:
18 landmarks on 134 standardized photographs of dental casts were digitized, and a Procrustes analysis was performed.
Results:
The size of the centroid in men was significantly larger than in women. Discriminant analysis with gender cross-validation did not show significant differences in the shape components. The variation pattern in the shape of the dental arches is mainly explained by PC1 (50.1% of the total variation, anteroposterior variation) and PC2 (13.3%, transverse variation).
Conclusions:
Given the morphological continuity that is observed when performing a statistical analysis of the variation pattern in shape and size of the arch applying geometric morphometric tools, the use of preformed templates for determining the shape of the dental arch should be reconsidered.
Keywords: (MeSh); dental arch; orthodontics; analysis, principal component
Objetivos:
Describir el patrón de variación de la forma de la arcada dentaria mandibular en una muestra de la Región Metropolitana mediante un estudio observacional, transversal.
Métodos:
Se digitalizaron 18 puntos de referencia en 134 fotografías estandarizadas de modelos de yeso y se realizó un análisis de Procusto para obtener los componentes de variación de la forma y el tamaño (tamaño del centroide= cs).
Resultados:
El tamaño de centroide en hombres es significativamente mayor que en mujeres. El análisis discriminante con validación cruzada no mostró diferencias significativas en los componentes de la forma según el sexo. Las diferencias en la forma de los arcos dentales, explicada por los dos primeros componentes de la forma correspondió al 73.4% de la varianza total (PC1= 50,14%, en el eje anteroposterior y PC2= 13,31% en el eje transversal).
Conclusiones:
De acuerdo con los resultados del presente estudio, se debe replantear el uso de plantillas preformadas en la determinación de la forma del arco dentario, dada la continuidad morfológica que se observa al realizar un análisis estadístico del patrón de variación en forma y tamaño del arco, como queda en evidencia al utilizar herramientas de morfometría geométrica.
Palabras clave: (MeSh); arco dentario; ortodoncia; análisis, componente principal
Objetivos
: Descrever o padrão de variação da forma do arco dentário mandibular em uma amostra populacional da Região Metropolitana, através de um estudo observacional transversal.
Métodos
: 18 pontos anatómicos em 134 fotografias padronizadas de moldes de gesso foram digitalizados e foi realizado uma análise Procrustes.
Resultados
: O tamanho do centróide nos homens é significativamente maior do que nas mulheres. A análise discriminante com validação cruzada de gênero não mostrou diferenças significativas nos componentes da forma. O padrão de variação na forma das arcadas dentárias é explicado principalmente por PC1 (50,1% da variação total, variação anteroposterior) e PC2 (13,3%, variação transversal).
Conclusões
: Dada a continuidade morfológica que se observa ao realizar uma análise estatística do padrão de variação da forma e tamanho da arcada, aplicando ferramentas morfométricas geométricas, o uso de templates pré-formados para determinação da forma da arcada dentária deve ser reconsiderado.
Palavras-chave: (MeSh); arcada dentária; ortodontia; análise, componente principal
Introduction
The study of dental arches has been relevant in fields such as anthropology and dentistry, and it has aimed at characterizing populations and establish normal ranges. In orthodontics, particularly in the therapeutic field, this study is of key importance, as one of its primary goals is to enhance the stability, functionality, and aesthetics of dental arches 1,2.
The shape of the dental arch refers to the geometry established by relating the alveolar process and the underlying basal bone with both intraoral and perioral forces 3,4. The alveolar process can be influenced by nutritional, functional, and systemic factors, which may alter the size, shape, and volume of this structure 5,6,1.
Various methods have been employed to study the shape of the dental arch. These include templates featuring predetermined geometric shapes, whereby arches are categorized based on their resemblance to such templates 2,7,8,9. More intricate approaches include functions such as the catenary curve, the cubic spline function, conic sections, polynomial functions including the quadratic polynomial and the sixth-degree polynomial, Euclidean distance matrices, Fourier series, and the beta function (4, 10).
A wide variety of preformed archwires are available in the orthodontic industry for use in patient treatment. The orthodontist selects and uses the preformed archwire shape that best suits each clinical case. Although this practice is very popular among clinicians, it overlooks the natural variation in dental arches within the population, as it conforms their shape to a pre-existing one (11. In view of these shortcomings, geometric morphometrics has been applied by some authors in the study of dental arch shape variation 5,12.
This morphological analysis tool has been primarily employed in the study of human populations by physical anthropologists and, more recently in dental practice to examine the dento-skeletal pattern of shape and size variation 13,14,15,16. This tool was developed for carrying out the statistical analysis of shape variation enabling the description, analysis, and comparison of the morphology of biological objects by differentiating the effect of shape variation from size variation, which is geometric in nature (centroid size = square root of the sum of the square distances from each landmark to the centroid point) 17,18,19,20,21,22). Thus, the form of a biological object is determined by both its size and the spatial or geometric relationship of the anatomical landmarks that comprise it 23.
Currently, the use of geometric morphometrics for the study of shape and size variation in the maxillofacial territory is undergoing a phase of expansion, with several publications already utilizing this morphological analytical tool 10,14,15,16. With this in mind, this study aims to describe the pattern of variation in the shape of the mandibular dental arch using geometric morphometrics standard pipeline in a population sample from the Metropolitan Region of Chile. Our null hypothesis states that changes in the shape of the mandibular dental arch occur solely by chance, regardless of factors such as the size of the dental arch or the sex of the individuals. This way, more precise information regarding its variability can be obtained, contributing to improve the orthodontic practice through personalized treatment.
Materials and Methods
This is an observational, cross-sectional study employing random sampling. The sample comprised 134 plaster models of the mandibular arch (67 women and 67 men), housed at the Center for Quantitative Analysis in Dental Anthropology (CA2) of the Faculty of Dentistry, Universidad de Chile. Inclusion criteria were as follows: well-preserved models from individuals with no history of surgical nor orthodontic treatment, complete dental arch (excluding third molars), fully erupted second molars, absence of cusp wear, no dental anomalies in size and/or shape, absence of evident asymmetries in the mandibular dental arch, and a Little's irregularity index 24) equal to or less than 3 mm. Sample size was calculated using an F test for overall MANOVA effects (total N= 128, alpha= 0.05, statistical power= 0.8, n groups= 2, effect size= 0.0625, Pillai's trace= 0.0588, G*Power program, v. 3.1.9.6).
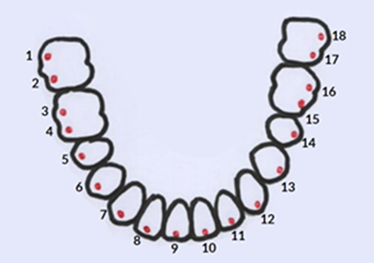
Standardized photographs were taken of each plaster model using a "Nikon" D3400 18-55 f/3.5-5.6G camera. The standardization of photographic registering involved employing a tripod to maintain camera stability at a consistent height and distance (50 cm) for all photos. Eighteen anatomical landmarks were digitized on each photograph based on the corresponding homology map (Table 1, Figure 1). These landmarks were digitized using the TPSDig2 program (v. 2.30; Rohlf, 2017), yielding an x, y matrix of landmark coordinates. Subsequently, the landmark coordinates were subjected to a generalized Procrustes Analysis (GPA) using the MorphoJ software, following a standardized geometric morphometrics pipeline 20,17.
Table 1. Definition of Landmarks in the Homology Map
| Landmark | Definition |
| 1 | Distobuccal cusp of the lower right second molar. |
| 2 | Mesiobuccal cusp of the lower right second molar. |
| 3 | Midbuccal cusp of the lower right first molar. |
| 4 | Mesiobuccal cusp of the lower right first molar. |
| 5 | Buccal cusp of the lower right second premolar. |
| 6 | Buccal cusp of the lower right first premolar. |
| 7 | Cusp of the lower right canine |
| 8 | Midpoint of the mesiodistal distance of the lower right lateral incisor. |
| 9 | Midpoint of the mesiodistal distance of the lower right central incisor. |
| 10 | Midpoint of the mesiodistal distance of the lower left central incisor. |
| 11 | Midpoint of the mesiodistal distance of the lower left lateral incisor. |
| 12 | Cusp of the lower left canine. |
| 13 | Buccal cusp of the lower left first premolar. |
| 14 | Buccal cusp of the lower left second premolar. |
| 15 | Mesiobuccal cusp of the lower left first molar. |
| 16 | Midbuccal cusp of the lower left first molar. |
| 17 | Mesiobuccal cusp of the lower left second molar. |
| 18 | Distobuccal cusp of the lower left second molar. |
Results
Intraobserver Error Calculation
The main author (FV) conducted the digitization of the 22 anatomical landmarks for 30 individuals, consisting of 15 females and 15 males. This process was repeated with the same individuals after a week. Subsequently, a Principal Component Analysis was performed separately for each group, using the shape components (PC1, PC2, ..., PCn) as linear variables in a one-way ANOVA (n= 60). The analysis only included the principal components that contributed to a cumulative variance corresponding to 90% of the total variance. Levene's test rejected the hypothesis of equal variances (p= 3.18E-19), leading to the application of the nonparametric Kruskal-Wallis test. This test revealed no statistically significant differences between the first and second measurements [H (Ji2): 1.714, Hc (corrected range): 1.714, p (equal groups): 0.944], confirming the absence of statistically significant observer bias in the measurements.
Sexual Dimorphism Analysis
Although, as anticipated, the centroid size (CSize) of men is significantly larger than that of women (CSize men = 10.71 +/- 0.56; Csize women = 10.28 +/- 0.55; t = 4.54, p = 1.271 E-05), there were no significant differences in the shape components concerning sex (discriminant analysis with cross-validation, correctly classified women = 62.7%; correctly classified men = 64.2% for expected values above 80%).
Pattern of Shape Variation Analysis
The observed pattern in the first two principal components of shape indicates anteroposterior contraction and expansion in PC1 (50.14% of the variance), while PC2 (13.31% of the variance) shows a pattern of transverse contraction and expansion of the dental arch (Fig. 2).
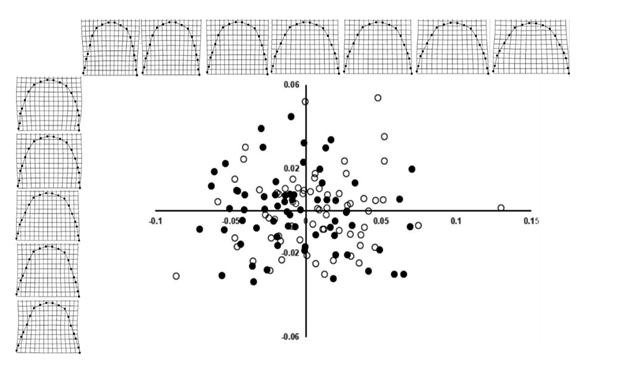
Figure 2: Shape Variation According to Principal Components 1 and 2 (PC1 = 50.14%, PC2 = 13.31%). The figures show the anteroposterior variation of the arch in the horizontal axis or PC1. The vertical axis (PC2) illustrates the transverse variation of the arch. Additionally, the absence of differences with respect to sex (females in white circles, males in black circles) is clearly observed.
In PC1, the landmarks exhibiting the greatest anteroposterior variation correspond to the buccal cusps of the second molar and the central incisors, while in PC2 they correspond to the buccal cusp of the second premolar and the distobuccal cusp of the second molar (Fig. 3).
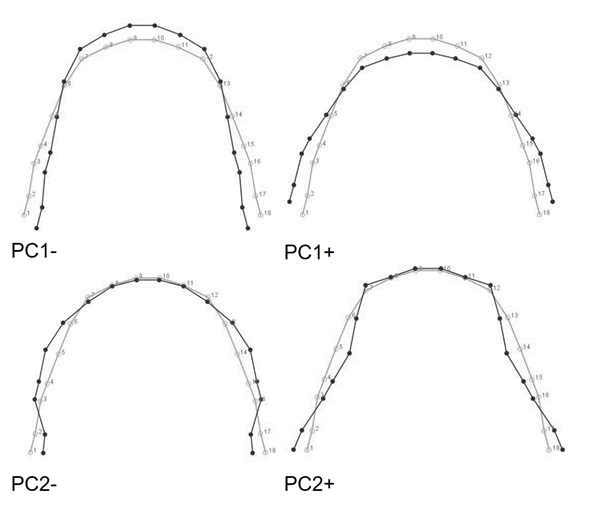
Figure 3: The above images depict overlays of the consensus configuration (in gray) with the extremes of variation (in black) in Principal Component 1 (PC1-, PC+). Primarily, differences in the sagittal dimension -attributed to variations in the position of the incisors- are observed. The lower images depict overlays of the consensus configuration (in gray) with the extremes of variation (in black) in Principal Component 2 (PC2-, PC+). The position of the second premolar and second molar accounts for the most significant variation observed along this axis.
Discussion
To investigate the variation of mandibular dental arch shape in a sample from the Metropolitan region of Santiago, Chile, a cross-sectional study was conducted using the standard geometric morphometrics pipeline. According to our findings, the centroid size of the mandibular arches is significantly larger in males compared to females. This difference is attributed to mesiodistal coronal size dissimilarity between the sexes, as previously reported (25, 26, 27, 28). However, as demonstrated in this study, when analyzing the arch shape itself independently from size, no statistically significant differences were observed between males and females. Other studies employing the same geometric morphometrics approach have also reported the absence of sexual dimorphism in dental arches (10, 11, 12).
Our main finding reveals a significant variability in the shape of the mandibular arch around the consensus shape, which is positioned at the center of the distribution graph, resembling the "ovoid" shape of preformed templates. This may explain why other authors, using preformed templates, have concluded that the most prevalent shape in the populations they studied is the ovoid shape 30.
Therefore, determining when a shape ceases to be "ovoid" and becomes classified as "round," "square," or "triangular" becomes arbitrary (31, 32). This fact is acknowledged in research employing the aforementioned definitions (33. According to our results, these shapes, supposedly represented in the mandibular arches of the population, are definitely not observed in the pattern of shape variation revealed by geometric morphometrics, which is primarily explained by differences in the positions of the second molars, incisors, and second premolars.
When using preformed templates for arch form studies, researchers must determine which template most accurately matches the shape of the dental arch under examination. Based on this assessment, they make a classification judgment by assigning a specific shape. As noted, we find this classification criterion to be arbitrary, as it fails to consider the natural variability in the shape of dental arches. The main challenge in orthodontic practice arises from the use of preformed arch wires, particularly the elastic or superelastic alloy arch wires offered to orthodontists by commercial manufacturers. In clinical practice, orthodontists select the preformed archwire that best fits the arch form of a particular patient. In a study of preformed archwires, only one out of ten commercial brands showed a close match to the average obtained (10. We believe that ideally, these preformed archwires should be customized from the outset of treatment, even those that are elastic or superelastic, to conform to the shape of the patient's dental arch. Failure to do so could potentially introduce a factor of instability or relapse (34.
In summary, there is significant variability in the shape of the mandibular arch around the consensus shape, resembling the "ovoid" form of preformed templates. Other shapes such as round, triangular, and square are deviations from the consensus shape and are primarily influenced by differences in the positions of the second molars and incisors. Consequently, geometric morphometrics reveals morphological continuity along both axes, thus not being able to precisely classify the dental arch as ovoid, square, round, or triangular.
REFERENCES
1. Proffit. Equilibrium theory revisited: factors influencing position of the teeth. Angle Orthod. 1978 Jul; 48(3):175-86. [ Links ]
2. Juárez, Venegas. Prevalencia de la forma de los arcos dentales en adultos con maloclusión y sin tratamiento ortodóncico. Revista odontológica mexicana, 2006 10 (3): 109-114. [ Links ]
3. O`Neil, Kau. Comparison of dental arch forms created from assessment of teeth, alveolar bone, and the overlying soft tissue. J orofac orthop, 2021 82: 413-421. [ Links ]
4. Yang, Li. Comparison of maxillary anterior mathematical proportions among 3 dental arch form. The journal of prosthetic dentistry, 2021. [ Links ]
5. Banabilh, Suzina, Dinsuhaimi, Samsudin, Singh. Dental arch morphology in south-east Asian adults with obstructive sleep apnoea: geometric morphometric. Journal of oral rehabilitation, 2009 36; 184-192. [ Links ]
6. Rainly. Craniofacial Growth, Dent Clin North Am. 2000, Jul; 44 (3):457-70. [ Links ]
7. Agurto, Sandoval. Morfología del arco maxilar y mandibular en niños de ascendencia mapuche y no mapuche. Int. J. Morphol, 2011 29(4):1104-1108. [ Links ]
8. Nojima, Mclaughlin, Isshiki & Sinclair. A comparative study of Caucasian and Japanese mandibular clinical arch forms. Angle Orthodontist, vol. 71, No. 3, 2001. [ Links ]
9. Bedoya, Osorio & Tamayo. Dental ach size, biting force, bizygomatic width and face height in three Colombian ethnic groups. Int. J. Morphol, 2015 33(1): 55-61. [ Links ]
10. Camporesi, Franchi, Baccetti & Antonini. Thin plate spline analysis of arch form in a southern European population with an ideal natural occlusion. European journal of orthodontics, 2006 135-140. [ Links ]
11. Wang, Xia, Jiayi Li, Lvyuan Li, Fei Yu, Yuan, Fang &Ye. Accuracy of dental arch form in customized fixed labial orthodontic appliances. AJO-DO, 2022 (162(2): 173-181. [ Links ]
12. Wen, Hai Ming Wong, Tao Pei & Mcgrath. Adolescent dental arch development among southern Chinese in Hong Kong: a geometric morphometric approach. Nature research, 2019 9:18526. [ Links ]
13. Singh, McNamara & Lozanoff. Spline analysis of the mandible in human subjects with Class III malocclusion. Archives of Oral Biology, 1997 42(5), 345-353. [ Links ]
14. Chang, Lin, Liu & Chang. Midfacial and mandibular morphometry of children with Class II and Class III malocclusions. Journal of Oral Rehabilitation, 2005 32(9), 642-647. [ Links ]
15. Franchi, Baccetti, Stahl & McNamara. Thin-plate Spline Analysis of Craniofacial Growth in Class I and Class II Subjects. The Angle Orthodontist, 2007 77(4), 595-601. [ Links ]
16. Díaz Muñoz & Manríquez Soto. Skeletodental Diagnosis Using a Geometric Morphometric Approach. International Journal of Odontostomatology, 2014 8(1), 05-11. [ Links ]
17. Rohlf. Morphometrics. Annu. Rev. Ecol. Syst. 1990. 21: 299-316 [ Links ]
18. Slice. Geometric Morphometrics. Annual Review of Anthropology, 2007 36(1), 261-281. [ Links ]
19. Toro Ibacache, Manríquez Soto & Suazo Galdames. Morfometría Geométrica y el Estudio de las Formas Biológicas: De la Morfología Descriptiva a la Morfología Cuantitativa. International Journal of Morphology, 2010 28(4), 977-990. [ Links ]
20 13 4(4), 393-399. [ Links ]
21 21. Benítez & Püschel. Modelando la Varianza de la Forma: Morfometría Geométrica Aplicaciones en Biología Evolutiva. International Journal of Morphology, 2014 32(3), 998-1008. [ Links ]
22. Mitteroecker & Schaefer. Thirty years of geometric morphometrics: Achievements, challenges, and the ongoing quest for biological meaningfulness. American Journal of Biological Anthropology, 2022 178(S74), 181-210. [ Links ]
23. Adams, Rohlf & Slice. A field comes of age: Geometric morphometrics in the 21st century. Hystrix, the Italian Journal of Mammalogy, 2013 24(1). [ Links ]
24. Little. The Irregularity Index: A quantitative score of mandibular anterior alignment. Am. J. of Orthod. Vol. 68 num. 5. 554- 56 [ Links ]
25. Brace & Ryan. Sexual dimorphism and human tooth size differences. Journal of Human Evolution, 1980 9(5), 417-435. [ Links ]
26. Guatelli-Steinberg, Sciulli & Betsinger. Dental crown size and sex hormone concentrations: Another look at the development of sexual dimorphism. American Journal of Physical Anthropology, 2008 137(3), 324-333. [ Links ]
27. Hattab, Al-Khateeb & Sultan. Mesiodistal crown diameters of permanent teeth in jordanians. Archives of Oral Biology, 1996 41(7), 641-645. [ Links ]
28. Shaweesh. Mesiodistal and faciolingual diameters of the permanent teeth in a Jordanian population. Archives of Oral Biology, 2017 73, 253-258. [ Links ]
30. Agurto & Sandoval. Morfología del Arco Maxilar y Mandibular en Niños de Ascendencia Mapuche y no Mapuche. International Journal of Morphology, 2011 29(4): 1104-1108. [ Links ]
31. Lombardo, Fattori, Molinari, Mirabella, Siciliani. Dental and alveolar arch forms in a Caucasian population compared with commercially available archwires. International Orthodontics, 2013; 11: 389-421. [ Links ]
32. Tajik, Mushtaq, Khan. Arch forms among different angle classifications a - study. Pakistan Oral & Dental Journal 2011 June 31(1). [ Links ]
33. Paranhos, Andrews, Jóias, Bérzin, Daruge, Triviño. Dental arch morphology in normal occlusions. Braz J Oral Sci. 2011 10(1):65-68. [ Links ]
34. Rossouw & Malik. The retention protocol. In Seminars in Orthodontics. 2017 23 (2), 237-248. [ Links ]
Data Availability The entire dataset supporting the findings of this study was provided in this article
Conflict of Interest Statement The authors declare no conflict of interest in the publication of the article
Authorship contribution a) Study conception b) Data acquisition c) Data analysis d) Results discussion e) Manuscript drafting and revision f) Approval of the final version of the manuscript Authorship and Collaboration Contributions: -FV has contributed to b, c, d, e, f -MI has contributed to c, d, e, f -AD has contributed to a, c, d, e, f -GM has contributed to a, c, d, e, f
Received: September 19, 2023; Accepted: December 26, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
