










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Links relacionados
Compartilhar

 Permalink
PermalinkOdontoestomatología
versão impressa ISSN 0797-0374versão On-line ISSN 1688-9339
Odontoestomatología vol.26 no.43 Montevideo 2024 Epub 01-Jun-2024
https://doi.org/10.22592/ode2024n43e334
Update
Epidemiology of Dental Fluorosis in 12-year-old adolescents: Systematic review.
1
 http://orcid.org/0000-0001-9760-0640
http://orcid.org/0000-0001-9760-0640
2
http://orcid.org/0000-0002-3124-4716
1 Departamento de Odontopediatría y Tratamiento de las Disgnacias, Sub-Unidad Académica Odontopediatría, Facultad de Odontología, Universidad de la República Verdi 4604. Montevideo. Uruguay. CP 11400ivannagu@gmail.com
2 Departamento de Odontopediatría y Tratamiento de las Disgnacias, Sub-Unidad Académica Odontopediatría, Facultad de Odontología, Universidad de la República
3 Departamento de Odontopediatría y Tratamiento de las Disgnacias, Sub-Unidad Académica Odontopediatría, Facultad de Odontología, Universidad de la República
4 Departamento de Odontopediatría y Tratamiento de las Disgnacias, Sub-Unidad Académica Odontopediatría, Facultad de Odontología, Universidad de la República
The prevalence of dental fluorosis presents great variability worldwide. Its analysis is necessary as part of epidemiological surveillance
Objective:
To know the available literature on the prevalence of dental fluorosis among 12 years-old in relation to the community fluoridation method used.
Methodology:
Two researchers carried out a systematic review of the literature without time limits following the PRISMA guidelines, using the Pubmed, Cochrane, Scopus, BVS and Google Schoolar databases in English, Spanish, Portuguese and Italian.
Results:
19 cross-sectional articles were included, 16 belonging to communities that use fluoridated water, one that use fluoridated salt and 2 that compare results between communities that use fluoridated water or salt.
Conclusions:
there is great variability in the reports of prevalence of dental fluorosis. Regardless of the community fluoridation method used, fluorosis lesions of mild severity are the most prevalent.
Keywords: Dental fluorosis; Fluorides; fluoridated salt; fluoridated water; adolescents
La prevalencia de fluorosis dental presenta una gran variabilidad a nivel mundial. Es necesario su análisis como parte de la vigilancia epidemiológica.
Objetivo:
Conocer la literatura disponible sobre prevalencia de fluorosis dental a la edad de 12 años en relación con el método de fluoruración comunitario utilizado.
Metodología:
Dos investigadoras realizaron una revisión sistemática de la literatura sin límites temporales siguiendo las pautas PRISMA, utilizando las bases de datos Pubmed, Cochrane, Scopus, BVS y Google Schoolar en idioma inglés, español, portugués e italiano.
Resultados:
Fueron incluidos 19 artículos de diseño transversal, 16 pertenecientes a comunidades que utilizan agua fluorurada, uno que utiliza sal fluorurada y 2 que comparan resultados entre comunidades que utilizan agua o sal fluorurada.
Conclusiones:
existe gran variabilidad en los reportes de prevalencia de fluorosis dental. Independientemente del método de fluoruración comunitario utilizado las lesiones de fluorosis de severidad leve son las más prevalentes.
Palabras clave: Fluorosis dental; Fluoruros; sal fluorurada; agua fluorurada; adolescentes
Os relatos sobre a prevalência de fluorose dentária aos 12 anos apresentam grande variabilidade, não havendo unificação quanto ao uso dos índices. Independentemente do meio comunitário de fluoretação e do índice utilizado, a fluorose dentária leve é a mais prevalente.
Objetivo:
Conhecer a literatura disponível sobre prevalência de fluorose dentária aos 12 anos em relação ao método comunitário de fluoretação utilizado.
Metodologia:
Dois pesquisadores realizaram uma revisão sistemática da literatura sem limites de tempo seguindo as diretrizes PRISMA, utilizando as bases de dados Pubmed, Cochrane, Scopus, BVS e Google Schoolar em inglês, espanhol, português e italiano.
Resultados:
Foram incluídos 19 artigos transversais, sendo 16 pertencentes a comunidades que utilizam água fluoretada, un sal fluoretada e 2 que comparam resultados entre comunidades que utilizam água fluoretada ou salgada.
Conclusões:
Há grande variabilidade nos relatos de prevalência de fluorose dentária. Independentemente do método de fluoretação comunitária utilizado, as lesões de fluorose de gravidade leve são as mais prevalentes.
Palavras-chave: Fluorose dentária; Fluoretos; sal fluoretado; água fluoretada; adolescentes
Introduction and Background
The mechanism of action of fluorides is based on regulating the mineral balance between the tooth and oral fluids, with their bioavailability at low concentrations in the oral environment being fundamental (1. Strategies to deliver fluorides to the oral cavity are classified as: community (water, salt, milk), individual (toothpastes and mouthrinses), professional (gels, varnishes, foams, etc.), or a combination of these 2. The community-based strategies are directly related to a progressive decrease in the prevalence of caries worldwide.
Community access to fluoride, through artificially fluoridated drinking water and salt, has proven to be an efficient public health measure to globally reduce dental caries 2. Regarding fluoridated milk, the Cochrane review conducted to evaluate the available evidence up to 2014 concluded that it could be beneficial in reducing caries levels in schoolchildren. However, more high-quality studies are needed to reach a definitive conclusion regarding the degree of benefit of this measure 3.
Sustained exposure to excess fluoride (beyond the recommended dose according to the World Health Organization) can be harmful, causing dental fluorosis (DF).
DF is a qualitative structural defect of enamel. It is a form of hypomineralization where the enamel exhibits more porous areas with a higher protein content (4,5. Clinically, the characteristic lesions of DF appear opaque and calcareous, reflecting the increased porosity of the affected enamel. Its prevalence varies between 13.4% and 76.4% worldwide, and specifically in Latin America, it ranges from 29.42% to 63.7% 6-9. It appears in its mildest severity levels across all program reports utilizing community fluoridation as a strategy (10-14.
Since 1991, Uruguay has implemented a table salt fluoridation program with a concentration of 250 mg/kg of sodium fluoride. However, we have no available reports of its monitoring (15. Two recently published studies have raised concerns within the scientific community of our country. One of them reports a high prevalence of fluorosis among 12-year-old schoolchildren in the Department of Montevideo (84.8%), where 98.8% of cases were classified as very mild or mild fluorosis, and only 1.2% as moderate or severe fluorosis (9. The second study highlights the wide variability in fluoride concentrations found in the analysis of domestic salt packages marketed in Montevideo, revealing the lack of program surveillance 16. Periodic monitoring of both the quality of fluoridation and its impact on the population would optimize the benefits and enhance the safety of this Public Health measure.
This study aimed to analyze the scientific evidence on the prevalence and severity of dental fluorosis among 12-year-old adolescents in relation to the community fluoridation method used.
Methodology
In 2022, a systematic review of the literature in Spanish, English, Portuguese, and Italian was conducted, identifying epidemiological studies on DF among 12-year-old adolescents in communities with salt or water fluoridation programs. The study followed PRISMA guidelines for design and publication (17 and was registered in the PROSPERO registry.
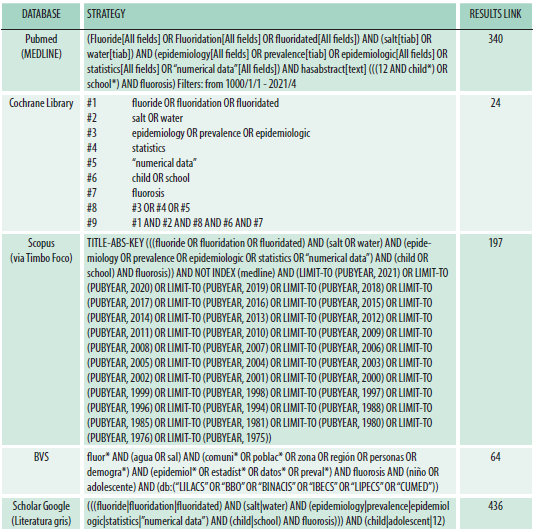
Search strategies were created to cover the following databases without time restrictions: PubMed (Medline, NCBI, USA), Cochrane Library (Cochrane Collaboration, including Cochrane Oral Health's Trials Register and the Cochrane Central Register of Controlled Trials (CENTRAL)), Scopus (via Timbo foco, the academic access platform of the University of the Republic of Uruguay and the National Agency for Research and Innovation), and the Virtual Health Library (PAHO/WHO) were utilized. The gray literature database Scholar Google was also included (Table 1).
All articles providing epidemiological data on fluorosis among 12-year-olds in communities with water fluoridation (WF) or salt fluoridation (SF) were included. Articles from communities with naturally fluoridated water were excluded.
Two reviewers (IG, SA) independently evaluated the identified publications. Duplicate papers were excluded, and selection by title and abstract was performed. After full-text reading, the final selection of articles was made according to the eligibility criteria. In cases of disagreement, two expert reviewers (LA, JL) solved the issue.
Results
The search strategy retrieved 1062 articles (437 from Google Scholar, after screening until no significant new words were found; 340 from PubMed; 197 from Scopus; 64 from BVS; 24 from Cochrane), of which only 512 were considered for abstract reading after eliminating duplicates and reviewing titles. To avoid overlapping data, only the most recent publication from the same research team was included. After reading the abstracts, 479 articles were excluded, resulting in 19 articles being included after full-text reading (Figure 1).
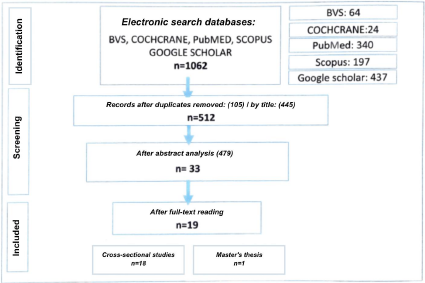
The included articles were all cross-sectional studies: 14 from Brazil, two from Europe (Switzerland and Ireland), one from Uruguay, one from the USA, and one from Asia (Singapore). Of all the included studies, 16 were conducted in communities using water fluoridation, one used fluoridated salt, and two compared communities using water or salt.
Fluorosis prevalence showed a very broad range between 0.5% and 84.1% globally and in Latin America between 0.5% and 58.9% 19,20.
Variations were observed in the indices used across the selected studies, each applied with different criteria. Thirteen studies employed the Dean index (DI) 18-30, while five utilized the Thylstrup Fejerskov index (TFI) 7,31-34, with one study comparing both (35. Among those employing the DI, 10 merged the "healthy" and "questionable" categories to signify the absence of DF (18,20-26,28,29, while 3 interpreted the "questionable" category as indicative of DF 27,30,33, 1 provided no specifications (19. A study correlated the TFI with the DI, considering the "questionable" category as indicative of DF 34.
Consensus among studies reporting on fluorosis severity indicates that mild and moderate lesions predominate, regardless of the community fluoridation method or index utilized (7,18,31,32,34,36,20-22,24,26,27,29,30(Table 2).
Discussion
This review aimed to assess available literature concerning epidemiological data on DF and the diagnostic indicators used at the age of 12.
Community water and/or salt fluoridation is a universal measure for preventing dental caries (DC) 37-39. It represents an equitable, cost-effective public health measure, offering lifelong oral health benefits to all community members and reducing disparities. The systematic review conducted by Iheozor-Ejiofor et al. in 2015, aimed at assessing the effects of fluoridated water on the prevention of DC and DF, concluded that the implementation of WF resulted in a 35% reduction in the extent of DC in primary dentition (DFT) and 26% in permanent dentition (DMFT) (40. The benefits of using SF in DC prevention were firmly established in the early 1980s, following numerous successful implementations of this measure in European and American countries 37.
Table 2. Selected articles regarding dental fluorosis at 12 years of age.
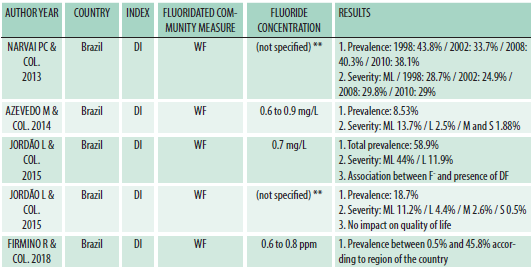
*International measurement system 1mg/L is equivalent to 1ppm.
** Brazil has had a water fluoridation program since 1974 with a concentration of 0.7 mg/L (Ministerio Da Saude 2009)
Concerns about the emergence of DF have always accompanied community fluoride measures. Dean's studies, conducted in US populations with varying concentrations of natural fluoride in water, demonstrated a clear correlation between fluoride concentration and the occurrence of DF with varying degrees of severity (41,42. The concentration recommended by the US Department of Health and Human Services in 1962, and internationally followed, ranged from 0.7 to 1.2 mg/L. Currently, this recommendation has been set at the lower limit of 0.7 mg/L, as evidence suggests that preventive benefits against dental caries remain intact while minimizing the risk of DF (43,44. The findings from the systematic review published in 2015 by the Cochrane group on water fluoridation suggest that at a fluoride level of 0.7 ppm, there is a 12% probability of developing DF 40. In this review, the prevalence of fluorosis exhibits a broad spectrum, ranging from 0.5% to 84.1% (18,19, and particularly in Latin America, from 0.5% to 58.9% 19,20. Such wide-ranging data, primarily sourced from Brazil, a nation employing WF as a community fluoridation method, may stem from variations in the criteria applied to the utilized indexes.
It is pertinent to consider the imperative of standardizing the use of indexes that are universally applicable and sensitive for coding DF. Such standardization would facilitate comparisons with reduced bias risks. Through a literature review, it became evident that the choice of indexes used exhibits significant variability: thirteen studies employed DI, five utilized TFI, one employed TFI while establishing a correlation with DI, and one utilized both, comparing them. This comparative analysis indicates that both indexes can identify DF prevalence similarly, with TFI demonstrating greater specificity in recording the severity of DF 35. Additionally, among the studies conducted with the DI, ten merge the "healthy" and "questionable" categories as the absence of DF, two consider the "questionable" category as the presence of DF, and one does not specify the criterion used. These variations in the assessment and classification of DF determine numerous limitations in terms of prevalence data and comparison of findings. This complexity impedes the collaborative efforts of scientific communities in analyzing and measuring the impact, thus hindering the achievement of standardized preventive measures considered universal.
SF has been demonstrated to have a comparable impact on oral health as the aforementioned method, with the added advantage of its elective incorporation into the diet. However, its consumption may face certain limitations related to its vehicle, considering the WHO recommendations for cardiovascular disease prevention 37,39. The recommended fluoride concentration for salt intended for human consumption ranges from 200 to 250 mg/kg 37. In this review, prevalence data of DF in studies conducted in communities using SF vary between 19.4% and 45% 27,34. Regarding this variation, it is important to note that the study reporting a lower prevalence only evaluates the anterior teeth, while the other includes all dental pieces. Thus, this variation is expected because at the age of 12, natural wear on the anterior teeth may lead to underestimated prevalence. Studies evaluating DF based on TFI report a higher prevalence 32,34 compared to those using DI 27. This difference could be attributed to the prophylaxis and drying procedures carried out prior to TFI evaluation, which are not conducted with DI, potentially leading to an underestimation of DF presence.
It can be asserted that DF in its very mild and/or mild degrees is the sole undesirable effect of community fluoride use measures (14. Eighteen studies included in this review indicate that the mildest forms of DF are the most prevalent. When comparing severity reports based on the index used, it is notable that "very mild" fluorosis is reported as the most prevalent in ten studies utilizing DI 20-23,26-30,35, while studies employing TFI identify TFI 1 and 2 as the most prevalent severity levels 7,31-35.
Nine studies conclude that due to the way DF presents itself, it is not self-perceived as an aesthetic issue and thus is not considered a public health concern 20,22,25-27,29,31,32,45.
Conclusions
Analysis of the studies included in this review reveals considerable variability in reporting the prevalence of DF. One possible explanation for this finding is the lack of standardized criteria regarding the index used or its application method, which hinders the comparison of study results.
Mild DF is consistently the most prevalent form, irrespective of the community fluoridation method or the index employed. Since this mild presentation of DF is generally not perceived as an aesthetic problem, it is unlikely to impact individuals' quality of life significantly.
Joint efforts among scientific communities are imperative in analyzing and assessing the impact of this public health intervention to maximize its benefits and ensure safety.
REFERENCES
1. Tenuta, L., & Cury J. Fluoruro: De la ciencia a la práctica clínica. In: Amolca, editor. Tratado de odontopediatría. 1a ed. Bogota; 2008. p. 149. [ Links ]
2. Tenuta LMA, Cury JA. Fluoride: Its role in dentistry. Braz Oral Res. 2010;24(SUPPL. 1):9-17. [ Links ]
3. Yeung CA, Chong LY e., Glenny AM. Fluoridated milk for preventing dental caries. Cochrane database Syst Rev. 2015;9(9):CD003876. [ Links ]
4. Drummond BK, Kilpatrick N. Planning and Care for Children and Adolescents with Dental Enamel Defects: Etiology, Research and Contemporary Management. 2015. 1-175 p. [ Links ]
5. Fejerskov O, Manji F, Baelum V. The nature and mechanisms of dental fluorosis in man. J Dent Res. 1990;69(SPEC. ISS. FEB.):692-700. [ Links ]
6. Barbachan e Silva B, Maltz M. Prevalence of dental caries, gingivitis, and fluorosis in 12-year-old students from Porto Alegre -- RS, Brazil, 1998/1999. Pesqui Odontol Bras. 2001;15(3):208-14. [ Links ]
7. Benazzi AS, da Silva RP, de Meneghim M, Ambrosano GM, Pereira AC. Dental caries and fluorosis prevalence and their relationship with socioeconomic and behavioural variables among 12-year-old schoolchildren. Oral Health Prev Dent (Internet). 2012;10(1):65-73. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22908090 [ Links ]
8. Michel-Crosato E, Raggio DP, Coloma-Valverde ANDJ, Lopez EF, Alvarez-Velasco PL, Medina MV, et al. Oral health of 12-year-old children in Quito, Ecuador: A population-based epidemiological survey. BMC Oral Health. 2019;19(1):1-10. [ Links ]
9. Angulo M, Cuitiño E, Molina-Frechero N, Emilson CG. The association between the prevalence of dental fluorosis and the socio-economic status and area of residence of 12-year-old students in Uruguay. Acta Odontol Scand (Internet). 2020;78(1):26-30. Available from: https://doi.org/10.1080/00016357.2019.1642514 [ Links ]
10. Calado R, Ferreira CS, Nogueira P, Melo P. Caries prevalence and treatment needs in young people in Portugal: the third national study. Community Dent Health. 2017;34:107-11. [ Links ]
11. Mittal M, Chaudhary P, Chopra R, Khattar V. Oral health status of 5 years and 12 years old school going children in rural Gurgaon, India: An epidemiological study. J Indian Soc Pedod Prev Dent. 2014;32(1):3-8. [ Links ]
12. Narbutaite J, Virtanen JI, Vehkalahti MM. Variation in fluorosis and caries experience among Lithuanian 12 year olds exposed to more than 1 ppm F in tap water. J Investig Clin Dent. 2016 May;7(2):187-92. [ Links ]
13. Zhou Y, Chen DR, Zhi QH, Tao Y, Wang X, Feng XP, et al. The Prevalence and Associated Risk Indicators of Dental Fluorosis in China: Findings from the 4th National Oral Health Survey. Chin J Dent Res. 2018;21(3):205-11. [ Links ]
14. Toumba KJ, Twetman S, Splieth C, Parnell C, van Loveren C, Lygidakis N. Guidelines on the use of fluoride for caries prevention in children: an updated EAPD policy document. Eur Arch Paediatr Dent (Internet). 2019;20(6):507-16. Available from: https://doi.org/10.1007/s40368-019-00464-2 [ Links ]
15. Decreto N° 375/990 17 de Agosto de 1990, Plan nacional de fluoracion de la sal para consumo humano patologia bucal, (IMPO 10 de setiembre de 1990) (Internet). Available from: http//www.impo.com.uy/bases/decretos/375-1990 [ Links ]
16. Dall Onder A, Fabruccini A, Alvarez L, Hashizume L. Paula A. Concentración de fluoruros en la sal de uso doméstico comercializada en Montevideo, Uruguay. Odontoestomatol. 2021;23(38):1-8. [ Links ]
17. Urrutia G, Bonfill X. Declaración PRISMA: una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis (Internet). Medicina Clínica. 2010;135: 507-11. Available from: http://es.cochrane.org/sites/es.cochrane.org/files/public/uploads/PRISMA_Spanish.pdf [ Links ]
18. Lo GL, Bagramian RA. Prevalence of dental fluorosis in children in Singapore. Community Dent Oral Epidemiol. 1996;24(1):25-7. [ Links ]
19. Firmino RT, Bueno AX, Martins CC, Ferreira FM, Granville-Garcia AF, Paiva SM. Dental caries and dental fluorosis according to water fluoridation among 12-year-old Brazilian schoolchildren: a nation-wide study comparing different municipalities. J Public Heal (Internet). 2018;26(5):501-7. Available from: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85053304094&doi=10.1007%2Fs10389-018-0901-0&partnerID=40&md5=ec598e48ed1009f13812cc3713c98c47 [ Links ]
20. Moimaz SA da. S, Saliba O, Marques LB, Garbin CAS alib., Saliba NA da. Dental fluorosis and its influence on children's life. Braz Oral Res. 2015;29(1):1-7. [ Links ]
21. Narvai PC, Antunes JLF, Frias AC, Soares M da C, Marques RA de A, Teixeira DS da C, et al. Fluorose dentaria em criancas de Sao Paulo, SP, 1998-2010. Rev saúde pública (Internet). 2013;47(supl.3):148-53. Available from: http://www.scielosp.org/scielo.php?script=sci_arttext& [ Links ]
22. Azevedo MS, Goettems ML, Torriani DD, Demarco FF. Factors associated with dental fluorosis in school children in southern Brazil: a cross-sectional study. Braz Oral Res. 2014;28(1):1-7. [ Links ]
23. Jordão LMR, Vasconcelos DN, Moreira R da S, Freire M do CM. Dental fluorosis: prevalence and associated factors in 12-year-old schoolchildren in Goiânia, Goiás. Rev Bras Epidemiol. 2015;18:568-77. [ Links ]
24. Leverett D. Prevalence of dental fluorosis in fluoridated and nonfluoridated communities-a preliminary investigation. J Public Health Dent. 1986;46(4):184-7. [ Links ]
25. Moysés SJ, Moysés ST, Allegretti AC V, Argenta M, Werneck R. Dental fluorosis: Epidemiological fiction? . Rev Panam Salud Publica/Pan Am J Public Heal (Internet). 2002;12(5):339-46. Available from: https://www.scopus.com/inward/record.uri?eid=2-s2.0-0036850627&doi=10.1590%2FS1020-49892002001100008&partnerID=40&md5=f918d2a38bd6afc99b597eb4914a3e01 [ Links ]
26. Cypriano S, Pecharki GD, de Sousa M da LR, Wada RS. (Oral health of schoolchildren residing in areas with or without water fluoridation in Sorocaba, São Paulo State, Brazil). Cad Saude Publica. 2003;19(4):1063-71. [ Links ]
27. Sagheri D, McLoughlin J, Clarkson JJ. The prevalence of dental fluorosis in relation to water or salt fluoridation and reported use of fluoride toothpaste in school-age children. Eur Arch Paediatr Dent. 2007 Mar;8(1):62-8. [ Links ]
28. Ditterich RG, Portero PP, Gabardo MCL, Wambier DS. Prevalência de fluorose dentária e de opacidades de origem não-fluorótica em áreas com e sem fluoretação artificial da água de abastecimento público TT - Prevalence of dental fluorosis and enamel opacities in areas with and without artificial fluoridatio. Arq odontol (Internet). 2008;44(2):11-7. Available from: https://periodicos.ufmg.br/index.php/arquivosemodontologia/article/view/3465/2240 [ Links ]
29. Moro L, Varaschini ÉL, Bighetti TI, Castilhos ED de. Condições de saúde bucal de escolares de 12 anos de idade, município de Água Santa, Rio Grande do Sul, Brasil TT - Oral health status of 12 year-old school children in Água Santa, Rio Grande do Sul, Brazil. Rev Fac Odontol Porto Alegre (Internet). 2009;50(2):13-8. Available from: http://seer.ufrgs.br/RevistadaFaculdadeOdontologia/article/view/8973/11498 [ Links ]
30 30. Rigo L, Caldas Junior A de F, Souza EA de, Abegg C, Lodi L. Estudo sobre a fluorose dentária num município do sul do Brasil TT - Study on the dental fluorosis in a Southern city of Brazil. Ciênc saúde coletiva (Internet). 2010;15(supl.1):1439-48. Available from: http://www.scielo.br/scielo.php?script=sci_arttext& [ Links ]
31 31. Franzolin S de OB, Gonçalves A, Padovani CR, Francischone LA, Marta SN. Epidemiology of fluorosis and dental caries according to different types of water supplies TT - Epidemiologia da fluorose e cáries dentárias de acordo com diferentes tipos de abastecimento de água. Ciênc saúde coletiva (Internet). 2010;15(supl.1):1841-7. Available from: http://www.scielo.br/scielo.php?script=sci_arttext& [ Links ]
32. Büchel K, Gerwig P, Weber C, Minnig P, Wiehl P, Schild S, et al. Prevalence of enamel fluorosis in 12-year-olds in two Swiss cantons. Schweizer Monatsschrift fur Zahnmedizin = Rev Mens suisse d'odonto-stomatologie = Riv Mens Svizz di Odontol e Stomatol. 2011;121(7-8):647-56. [ Links ]
33. Ramires I, Pessan JP, Levy FM, Rodrigues MHC, Almeida BS de, Kato MT, et al. Prevalence of dental fluorosis in Bauru, São Paulo, Brazil. J Appl Oral Sci. 2007;15(2):140-3. [ Links ]
34. Angulo M, Bianco P, Cuitiño E. Relevamiento y análisis de Caries Dental, Fluorosis y Gingivitis en adolescentes escolarizados de 12 años de edad en la República Oriental del Uruguay. 2010. [ Links ]
35. Provenzano MGA. Prevalência de cárie e fluorose dentária em escolares do município de Ibiporã-PR (Internet). 2003. p. 231. Available from: http://www.teses.usp.br/teses/disponiveis/25/25133/tde-23062009-102228/publico/MariaGisetteAriasProvenzano.pdf [ Links ]
36. Ditterich RG, Rodrigues CK, Stadler Wambier D. O sal fluoretado como alternativa em saúde bucal coletiva: vantagens e desvantagens Salt fluoridation as an alternative in dental public health: advantages and disadvantages. Rev Inst Ciênc Saúde. 2005;23(3):231-4. [ Links ]
37. Estupiñán-Day S. Promoting oral health: the use of salt fluoridation to prevent dental caries. Washington: PAHO; 2005. [ Links ]
38. Marthaler TM, Petersen PE. Salt fluoridation - An alternative in automatic prevention of dental caries. Int Dent J. 2005;55(6):351-8. [ Links ]
39. Organization World Health, World Health Organization. Guideline: Sodium intake for adults and children. World Heal Organ (Internet). 2012;1-56. Available from: http://apps.who.int/iris/handle/10665/77985%5Cn [ Links ]
40 40. Iheozor-Ejiofor Z, Worthington H V, Walsh T, O'Malley L, Clarkson JE, Macey R, et al. Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev (Internet). 2015(6):CD010856. Available from: http://dx.doi.org/10.1002/14651858.CD010856.pub2 [ Links ]
41. Dean HT, Jr. FAA, Elvove E. Domestic Water and Dental Caries: V. Additional Studies of the Relation of Fluoride Domestic Waters to Dental Caries Experience in 4,425 White Children, Aged 12 to 14 Years, of 13 Cities in 4 States. Public Heal Reports. 1942;57(32):1155. [ Links ]
42 42. Dean HT. Classification of Mottled Enamel Diagnosis. J Am Dent Assoc (Internet). 1934;21(8):1421-6. Available from: http://dx.doi.org/10.14219/jada.archive.1934.0220 [ Links ]
43. Services U. D of HAH. U.S. Public Health Service Recommendation for Fluoride Concentration in Drinking Water for the Prevention of Dental Caries. Public Health Rep. 2015;130(August):318-31. [ Links ]
44. Whelton HP, Spencer AJ, Do LG, Rugg-Gunn AJ. Fluoride Revolution and Dental Caries: Evolution of Policies for Global Use. J Dent Res. 2019;98(8):837-46. [ Links ]
45. Narvai PC, Antunes JLF, Frias AC, Soares M da C, Marques RA de A, Teixeira DS da C, et al. Dental fluorosis in children from Sao Paulo, southeastern Brazil, 1998-2010. Rev Saude Publica. 2013;47:148-53. [ Links ]
Conflict of Interest Statement The authors declare no conflict of interest in the publication of the article.
Authorship and Collaboration Contributions Statement: a) Study conception b) Data acquisition c) Data analysis d) Results discussion e) Manuscript drafting and revision f) Approval of the final version of the manuscript IG has contributed to: a, b, c, d, e and f MSA has contributed to: b, c, d, e and f JL has contributed to: a, b, c, d, e and f LA has contributed to: a, b, c, d, e and f
Received: September 26, 2023; Accepted: May 07, 2024
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
